
 XIFIN’s business intelligence mobile app.New Coding Offers Big Benefits
XIFIN’s business intelligence mobile app.New Coding Offers Big Benefits
BY GARY TUFEL
On October 1, 2014, the ICD-9 code sets used to report medical diagnoses and inpatient procedures will be replaced by ICD-10 code sets. The transition to ICD-10 is required for all entities covered by the Health Insurance Portability and Accountability Act (HIPAA).
The challenge of pulling this off successfully is the most significant one facing clinical labs today, according to Dianna Powell, presales clinical consultant for lab products, Merge Healthcare, Chicago.
Because clinical labs can be a step removed from immediate and direct patient interaction and often don’t see patients or even medical records face-to-face, it’s even more challenging to include appropriate diagnostic codes on orders that don’t flow through to the laboratory information system (LIS) from hospital information systems (HIS) or electronic health record systems (EHR), she says.
After the fact, it can be even more difficult to get the necessary information. “Some smaller labs even hold specimens for as long as possible and don’t run blood tests until the proper information is obtained,” Powell says. “This can impact reference labs and lab managers, as well as hospital labs, and the reimbursement delays can be enormous. So proper and timely coding is vital.”
The solution? One option is systems that prompt physicians to include necessary data and that will not work unless such information is included.
“ICD-10 has huge significance. It quadruples the number of diagnostic codes, from about 17,000 ICD-9 codes to around 74,000 [ICD-10 codes],” Powell says. “This means that doctors need to be provided with the tools to help them transition from ICD-9 to 10. The new coding will be more specific to, and especially beneficial for, tracking specific disease.
“For example, take patients with an infection like Methicillin-resistant Staphylococcus aureus (MRSA),” she says. “We will be able to more clearly identify outbreaks by the use of more precise statistical data. It’s incredibly more specific.”
Merge Healthcare’s Merge Clinical Lab Solutions (Merge LabAccess and Merge LIS) provide scalable laboratory information systems and middleware connectivity to lab instruments, automating the entire lab process and providing central point administration. Referring physicians get lab results faster, lab efficiency and test volumes are improved, automated processes allow for complete patient records, and there are short learning curves for new staff.
Merge LIS offers integrated interfaces with billing and diagnostic systems, and prescreens lab orders to avoid miscodings and other errors. It uses data that has been gathered and passes it to other lab analyzers in an electronic format, and offers billing transcription reports that can be amended or corrected manually, if necessary. And although billing is not done directly, the system can flow the information through to systems that do. Other options include prescrubbing charges, editing data so it’s accurate and ensuring that charges will properly bill. And because ICD-9 and ICD-10 charges are so vastly different and have increased so much in number, a crosswalk feature is crucial to a successful transition to ICD-10 codes, Powell says. “For instance, codes for many heart diseases increased enormously during the useful life of the ICD-9 coding system and could be impossible to find unless you know them by memory,” she says. “By increasing the code set, ICD-10 provides for needed expansion and logical grouping of codes by diagnostic category.
“On the plus side, if a MRSA outbreak occurs, the statistics we gather with ICD-10 codes with billing data could help us to determine the source of the outbreak and track it,” Powell adds. “It’s much more precise data, in that it brings big challenges as well as big benefits.”
 |
“The future of labs is now more risk and less reward. On the risk side, there is far more oversight by the US Department of Health and Human Services Office of the Inspector General, starting with Recovery Audit Contractors (RAC) demonstration projects that turned into the full-fledged RAC audit program.” —Bill Taylor, chief marketing officer, XIFIN |
Finding a Port in the Storm
A perfect storm of challenges faces clinical labs in the billing and coding arena. They are numerous and formidable—and there will be more change in the next 2 years than our industry has seen in the last 20, says Bill Taylor, chief marketing officer, XIFIN Inc, San Diego.
“The future of labs is now more risk and less reward,” Taylor says. “On the risk side, there is far more oversight by the US Department of Health and Human Services Office of the Inspector General, starting with Recovery Audit Contractors (RAC) demonstration projects that turned into the full-fledged RAC audit program.
“Now the HIPAA Privacy, Security, and Breach Notification Audit Program is well under way, and providers have incurred billions of dollars in fines for Protected Health Information (PHI) breach penalties,” Taylor adds. “But more significantly, profit margins are shrinking drastically. Annual reimbursement rates will shrink 1.75% per year until 2015.”
And reimbursements are being slashed across the board. Pathologists, for instance, face a 52% reduction in the technical component (TC) reimbursement for CPT code 88305 in the surgical pathology family in the Centers for Medicare and Medicaid Services 2013 physician fee schedule. The new molecular pathology CPT codes will be placed on the Medicare clinical laboratory fee schedule, and the American Medical Association is deleting “stacked” codes for molecular pathology procedures from the CPT 2013 codebook, allowing the test-specific 2012 MPP codes to become the standard.
As of July 1, Aetna planned to lower its reimbursement rates for lab services for all health plans to equal only 45% to 50% of the national Medicare reimbursement rates, and Cigna has lowered its rates as well. Other entities have also announced changes in reimbursement rates. Health plans are increasingly putting payment responsibility on patients, often greatly reducing or eliminating labs’ ability to obtain payment/reimbursement. Organizations such as independent practice associations and integrated delivery networks are also lowering their reimbursement rates.
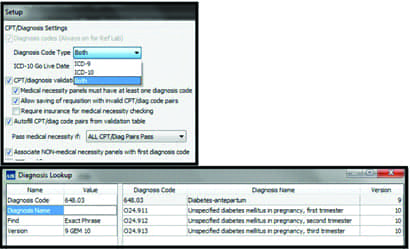 TOP: Shows how a user can select ICD-9 or ICD-10 as the active code set. BOTTOM: Shows the GEM (general equivalence mapping) of an ICD-9 code. Courtesy of CompuGroup Medical US. Some foresee a gloomy reimbursement outlook for clinical labs. Observers such as Robert Michel, editor-in-chief, DARK Daily, predict that providers with 4% to 6% profit margins won’t survive, and that some are already failing; so CEOs are desperately scrambling to maintain margins, Taylor says. Visibility and transparency are critical, and it’s really a strategic business intelligence problem, he says. “Our mantra is, ‘You can’t manage what you can’t measure,’ and right now, CEOs need the data and insights to optimize their businesses in this environment of shrinking margins,” Taylor says.
TOP: Shows how a user can select ICD-9 or ICD-10 as the active code set. BOTTOM: Shows the GEM (general equivalence mapping) of an ICD-9 code. Courtesy of CompuGroup Medical US. Some foresee a gloomy reimbursement outlook for clinical labs. Observers such as Robert Michel, editor-in-chief, DARK Daily, predict that providers with 4% to 6% profit margins won’t survive, and that some are already failing; so CEOs are desperately scrambling to maintain margins, Taylor says. Visibility and transparency are critical, and it’s really a strategic business intelligence problem, he says. “Our mantra is, ‘You can’t manage what you can’t measure,’ and right now, CEOs need the data and insights to optimize their businesses in this environment of shrinking margins,” Taylor says.
While the challenges are formidable, he offers another angle.
“These challenges, while significant, are surmountable,” Taylor says. “Focusing on billing information, such as which contracts and tests are being reimbursed and are profitable, for instance, is crucial. We are witnessing the severity of the situation in the conversations we’re having with laboratory CEOs every day.
XIFIN, which offers a cloud-based, revenue cycle management system for diagnostic service providers, had a record fourth quarter in 2012 and first quarter in 2013, Taylor says. The company has developed the first comprehensive accounts receivable and financial management solution for diagnostic service providers, designed specifically to address the problems that undermine the effectiveness and efficiency of laboratories’ revenue cycle management, he says.
Taylor says most labs of any size usually handle billing internally. “It’s not uncommon to see internal billing operations running at 4% to 6% of net revenue for routine clinical labs, and often as high as 10% to 15% for hospital, molecular, and pathology labs,” he says. “This is due to billing departments trying to handle their claim volume by throwing more labor at it. We like to see our clients operating at 2% to 4% of net revenue by automating as much of the process as possible, thus minimizing the labor component and eliminating clerical decision-making, a major source of cash leakage and compliance liability.”
In contrast, outsourced billing is a margin game, he says. “Paying 6% to 8% seems like a good deal if your internal operations are costing you 10%,” Taylor says. “But consider this. If a $100 claim is outsourced, the billing company receives $6. How much work can they really do on that claim and still make money for $6? As a result, they tend to write off more claims than you would with internal staff. The loss to the billing company is $6, but the loss to you is $100. In the end, it’s a false economy.”
Small startup labs are often focused on the clinical side of their business and optimizing laboratory processes, and don’t have the bandwidth to build out the billing IT infrastructure and staff, so outsourcing makes sense. However, as indirect providers, labs are completely dependent on ordering physicians, and as volume increases, labs want to manage their relationship with those physicians and with patients, which are easier to manage when billing and coding is done with in-house staff.
“We are a unique hybrid model,” Taylor says of XIFIN. “We maintain the IT infrastructure, the hardware, software, and all of the system edits, while the lab’s billing staff accesses the system through a standard web browser. Through use of a rules-based automated workflow, we minimize the laborcomponent of the billing process.”
 |
“The ICD-10 code sets are not a simple update of the ICD-9 code set. There are many more ICD-10 CM codes, and the descriptions are more complex.” —Sandy Laughlin, product manager, CompuGroup Medical US |
Easing the Transition to ICD-10
Many labs handle billing and coding internally with certified coders and properly trained billing staff who stay abreast of the changes to industry requirements, says Sandy Laughlin, product manager, CompuGroup Medical US, Boston. Billing through internal resources can be less costly than hiring a billing service to process lab coding, claim submission, and accounts receivables. Alternatively, Laughlin says, many labs outsource their billing because they don’t have the expertise to code, bill, and proactively handle the accounts receivable to maximize reimbursements.
In the mix, health care is also experiencing a shift from the traditional fee-for-service (FFS) model to payment models based on patient outcomes, Laughlin says. This comes in the form of an increasing presence of Patient Centered Medical Homes (PCMHs) and Accountable Care Organizations (ACOs). As these value-based models start gaining traction, labs need to evaluate their test volumes and payment arrangements for the new guidelines. Lab tests play a pivotal role in the diagnostic process, and contribute to the overall success of treatment plans. With the new models, treatment plans resulting in improved patient outcomes, improved quality of care, and reduced costs will be rewarded.
To prepare for what lies ahead, facilities should establish time lines with vendors and partners to test and transition to the ICD-10 code set, Laughlin says. “The ICD-10 code sets are not a simple update of the ICD-9 code set. There are many more ICD-10 CM codes, and the descriptions are more complex,” she says. “A LIS should provide tools to help the laboratory with the ICD-10 transition. For example, if an ICD-9 code is entered when creating a requisition, LabDAQ LIS will display the ICD-9 to ICD-10 mapping so that the user can select from a list of suggested ICD-10 codes that link to the ICD-9 code entered. This is just one example of how rules-based technology can assist in managing these complex changes.”
And while laboratory information systems are not billing systems, they may offer tools to assist with the billing and coding process, Laughlin says. Medical necessity checking can be completed in the LIS to ensure that the correct diagnosis codes are provided. These codes can be added/corrected prior to claim submission. A LIS can also assist with routing lab tests to the appropriate laboratory based on the patient’s insurance. With the routing of tests, labs won’t be performing tests that will not be reimbursed. Exporting charge or billing data in the HL7 standard format provides interoperability among systems.
These exports ensure that there is no missing or incorrect information, such as insurance, tests, CPT codes, and ICD-9 codes, she says.
CompuGroup’s LabDAQ LIS is currently exporting charge/billing information to the majority of the certified EHR systems and most stand-alone billing systems. Rules throughout the process help ensure a clean claim is created. In response to customer demand, the company has developed CGM DAQBILLING, a practice-management solution. Its tight integration with LabDAQ makes it an ideal companion product to efficiently handle the entire process from order to results to claim submission, Laughlin says. CGM DAQBILLING is based on a user-friendly web platform, and provides an integrated scheduler, electronic claims submission, online payor rules, and accounts receivable management. The ASP technology allows easy accessibility, data redundancy, and low startup costs. “This allows the billing office to focus on collections, not filing claims,” Laughlin says.
Gary Tufel is a contributing writer for CLP. For more information, contact Editor Judy O’Rourke, [email protected]



{kind=link}