
Supporting population health initiatives can demonstrate lab value
Accountable Care Organizations (ACOs) are playing important roles in reshaping the healthcare sector of the future. The excerpts below, from the research report Laboratory Services in Accountable Care Organizations, by Jenny Xu, PhD, published by G2 Intelligence, examine strategies that clinical laboratories can adopt in order to contribute value and thrive in this emerging environment.1—Ed.
Accountable Care Organizations (ACOs) were formed after the passage of the Patient Protection and Affordable Care Act (PPACA) on March 23, 2010.1 Three pillars, commonly referred to as the “Triple Aim,” define the ultimate goals of ACOs:2
- Improve patient experience of care.
- Improve the health of populations.
- Reduce the per capita costs of care.
To meet the Triple Aim, ACOs must develop effective value-based integrated care delivery models and adopt new payment arrangements.
ACOs progressed from concept to practice beginning before the passage of PPACA. In 2005, to test the concept of coordinated care, Medicare launched 10 physician group practice (PGP) demonstration projects, representing 5,000 physicians and 220,000 Medicare beneficiaries. In 2009, commercial payors also started ACO-like pilot projects, such as the Brookings-Dartmouth ACO pilot program.
After the passage of PPACA, a series of formal ACOs was launched, starting with Medicare Pioneer ACOs formed in December 2011 among providers with some prior experience in delivering integrated care. In April 2012, Medicare launched the first cohort of the Medicare Shared Savings Program (MSSP) ACOs among providers with little prior experience in integrated care delivery. Medicare also introduced the Advance Payment ACO Model and the ACO Investment Model to support providers such as smaller physician practices and rural hospitals that lack sufficient funds to invest in accountable care infrastructure, such as health information technology (HIT).
When Medicare was actively experimenting with shared savings ACOs, commercial payors ramped up their formation of ACOs, some modeled after Medicare shared savings and others with pay-for-performance, bundling, and capitation payment arrangements. By end of 2013, almost all major commercial payors had launched their own ACOs.
ACO CHANGES IN LABORATORY SERVICES
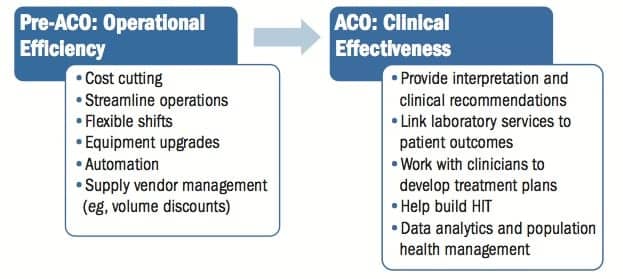
Figure 1. ACO laboratory initiatives shift focus from efficiency to effectiveness. Source: G2 Intelligence; Clinical Laboratory Management Association.
Since their inception, many ACOs have implemented changes in various facets of their operations to facilitate care coordination and achievement of the Triple Aim. Laboratories have reported experiencing both structural changes and financial changes (see Figure 1).
Structural Changes. Fears that many ACOs would close their laboratories and outsource laboratory services to third-party vendors as a way to control costs have not borne out. Very few ACOs (4.2%) report having closed their laboratories. Many laboratories (77.3%), however, report having experienced changes since joining ACOs.
G2 Intelligence surveys found that 22.7% of ACOs consolidated laboratories by merging multiple sites into one. Some ACOs (19.3%) also consolidated reference testing by sending out tests to fewer laboratories than before. Other ACOs are in the process of consolidating health information systems to improve connectivity and interoperability.
In addition to consolidation, some ACOs (21.8%) switched one or more laboratory contracts to lower-cost providers, particularly to national leading independent laboratories, accounting for about two-thirds of the switches.
Financial Changes. Major financial changes among laboratories in ACOs include reimbursement cuts, laboratory budget cuts, and shift toward value-based payment models.
Reimbursement cuts are a prevailing theme for laboratories and for healthcare services across the board. For laboratories, both Medicare and commercial payors are lowering reimbursement rates across testing categories. Laboratory budget cuts also pose financial challenges for laboratories, with 22.7% of laboratories reporting budget cuts since joining ACOs.
Reforms in care delivery and payment go hand in hand. As ACOs are pursuing more effective, value-based care delivery models, they are also adopting new value-based payment arrangements with payors. Several different value-based payment models have emerged and are used in ACOs and across the wider healthcare system, including pay-for-performance, shared savings programs, bundled or episode-based payments, and capitation.
These new payment models share two common features: greater financial risk assumed by providers and increasing scope of services covered per payment unit. To be eligible for bonus payments under shared savings arrangements, ACOs must meet both savings targets and quality requirements. The contracts with payors, however, do not determine how savings should be allocated among various service providers within ACOs.
ACO LABORATORY VALUE INITIATIVES
G2 Intelligence surveys reported that more than three-quarters of laboratory directors (76.6%) did not think their laboratories were receiving proper financial compensation for their value contributions made to ACOs. One way to improve the likelihood of laboratories receiving proper financial compensation for their contributions is to prove the value of laboratory services to ACOs through initiatives that help ACOs achieve the Triple Aim.
Not all laboratory initiatives are perceived as being equally valuable to ACOs, according to G2 Intelligence surveys. Initiatives directed to patient care are more effective value differentiators than efficiency-focused initiatives. Initiatives directed to patient care include integrating clinical recommendations into laboratory reports; providing post-test interpretation consultation on complex tests; and working with clinicians to develop treatment plans, if needed, all of which assist clinicians in making better decisions. In the process of providing clinical decision support, laboratories are also linking their services to patient outcomes, which helps generate evidence for the value of laboratory services.
In addition to the initiatives directed to patient care, laboratories can help build an effective HIT infrastructure. Given that 70% of the data stored in the electronic health record (EHR) is laboratory data, and laboratory data contributes to more than 70% of clinical decisions, laboratories are well positioned to provide innovative solutions to connectivity and interoperability, two key features required to enable the delivery of coordinated care.3
Laboratories can also contribute value to risk identification and stratification, monitoring and tracking patient health, and identifying and managing care gaps, three core activities involved in population health management.
Laboratories play a significant role in developing predictive analytics to support population health. Many ACOs are approaching population health management as a two-phase implementation, targeting the most expensive patients—including those with multiple chronic conditions—first. With the transition to population health 2.0, many ACOs will apply predictive analytics to a broader range of patients to proactively identify those in need of care.4 This means the demand for data analytics will be even greater as ACOs mature.
While the need for analytics is widely recognized, few hospitals are equipped with this capability. In 2013, only 18% of hospitals used predictive analytics in care coordination.5 As a result, the potential opportunities for laboratories to engage analytics are enormous, given their invaluable experience with analytics used in laboratory information systems (LIS) already.
PROVIDE VALUE TO POPULATION HEALTH MANAGEMENT
Managing population health is one of the three pillars supporting ACOs’ Triple Aim. With population health management, healthcare providers proactively engage with patients, prompting them to stay healthy either through preventive measures or by effectively managing existing conditions, which reduces the occurrence of catastrophic events and the need for costly acute care.6 The savings potential of an ACO will not be fully achieved without population health management (see Figure 2). Population health management entails three core activities:7
- Risk identification and stratification.
- Identifying and managing care gaps.
- Monitoring and tracking patient health.
Identify and Manage At-Risk Populations. Risk identification and stratification are critical to population health management given the significantly higher healthcare costs consumed by at-risk patients. Research shows that almost half of healthcare spending goes to the care of just 5% of the population, whereas the spending by the lowest 50% of spenders totaled just 3% of all healthcare expenditures.8
Chronic conditions exacerbate spending. According to the CDC, 75% of healthcare costs go toward the treatment of chronic diseases.9 Patients with multiple chronic conditions cost seven times more than healthy patients.8 Patients with multiple chronic diseases not only pose significant financial risks to payors and providers, they also present significant opportunities for cost savings when managed properly. They are 100 times more likely to have an avoidable hospitalization, or to have duplicate laboratory tests ordered.
Multiple chronic conditions are prevalent among patients in the United States, particularly among the elderly. In 2010, about two-thirds of Medicare enrollees had multiple chronic conditions, accounting for approximately 94% of Medicare spending.10 Chronic diseases currently affect 133 million people in the United States and are expected to increase by 37% in the coming decades.11
This population of high-risk patients is of key concern for ACOs. To keep costs in control, many ACOs have started identifying patients with the highest risks both clinically and financially, such as those with multiple chronic conditions, and are working to manage their conditions more effectively to minimize avoidable complications, hospitalizations, and declines in health conditions. This is a distinct departure from the care delivery model centered on acute care that has emerged from the volume-driven fee-for-service payment model.12 Without payment reform, population management strategies such as risk stratification and efforts to improve the management of chronic conditions would not be rewarded.
Laboratory data is an important input to risk stratification, along with pharmacy data, claims data, and other information. Laboratory results may also be effective at stratifying patients with specific conditions. In one study, 2,370 patients with coronary artery disease (CAD) were stratified based on clinical variables and laboratory results, such as high-density lipoprotein, neutrophil-to-lymphocyte ratio, and FT3 serum level. The variables had prognostic value, showing stratification of three risk groups: 84%, 57%, and 41% increase in rate of cardiac events.13
Other research suggests that risk stratification using laboratory data could be valuable in managing the health of patients with non-healing skin ulcers, common among patients with chronic diseases such as diabetes, kidney disease, peripheral neuropathy, and peripheral arterial disease. Hemoglobin levels, white blood cell counts, and albumin levels could be used to predict poor outcomes and identify patients who need more aggressive care.14
Laboratory data analytics could also help identify “time bombs.” At the University of Miami, pathologist Philip Chen tried to identify high-risk diabetic patients using the longitudinal data in the LIS. His analysis found that the top 5% of spenders were not always the most expensive. Rather, 3% transitioned from lower spending cohorts to the highest spending cohort each year. These “time bombs” tend to be poorly managed diabetics that progress to myocardial infarction.15 Dynamic updates of risk stratification could help identify these 3% of patients earlier to enable proper interventions to prevent them from moving on to the highest spending group.
These examples suggest that laboratories have a real opportunity to get involved with population health management by contributing data to risk stratification, creating a strategy for dynamic updates of risk stratification, and providing clinical decision support to effectively manage high-risk patient groups.
According to G2 Intelligence surveys, 50.7% of laboratories have started identifying high-risk patients for the ACOs and there is plenty of room for improvement. G2 Intelligence interviews suggest that laboratory engagement with ACOs to define risk stratification strategies and opportunities is still lacking. “We are working with another health system which has already developed a number of risk stratification formulas, and we are really relying on them. We are not starting from scratch with our own pathologists to help us with risk stratification profiles,” said the chief operating officer at a large health system ACO. “Not yet at least. Maybe in the future.”
Identify and Manage Care Gaps. Another core activity in population health management is identifying and managing care gaps. Care gaps exist in several areas:16
- Prevention. If the goal is to get a population of women to receive a mammogram each year, intervention such as office-based decision support will be needed for women who do not see their physicians on their own.
- Chronic disease. Diabetic patients with high A1c levels (7–8) need to be managed more closely to prevent the occurrence of expensive episodes.
- Unclosed loops. An abnormal test result needs to be followed up on and referral gap management may be required to close the loop.
- Medication safety. Monitoring may be needed to adjust doses and check efficacy and laboratory gap management may be required to ensure proper monitoring.
- Regular care failures. Patients whose conditions decline despite intervention may need care plan alterations.
By monitoring care gaps in focal areas, providers can apply interventions to close the gaps quickly. Care gap management has proven to effectively improve patient outcomes. Cigna compared patients who received care from embedded care coordinators responsible for facilitating interventions to patients who received standard care at its Dartmouth-Hitchcock ACO and found that care gap management led to a 10.4% overall improvement in gap closing rate in 6 months, including a 13.8% improvement for high priority patients, 16% for hypertension patients, and 8.1% for diabetes patients.17
One effective way to watch for care gaps is use of care gap reports. These reports pull information from an ACO’s HIT and identify cases where care protocols and goals are not being met, often determined based on laboratory results as key data points. The reports aim to not only improve quality by closing care gaps, but also streamline processes so that care is delivered more efficiently.18 Laboratories can contribute to care gap management by identifying laboratory data that indicates care gaps, and monitor risk factors through analyzing and tracking laboratory results.
Care gap management may also assist with public health initiatives, such as infectious disease screening, in ways that translate into value for ACOs by identifying patients in need of care.19 Laboratories can play an active role in care gap management by helping define laboratory data that can be used to identify patients in need of care, to track patient health status, and to generate metrics that indicate the closing of care gaps.
Monitor Individual Patient Health and Population Health. Laboratory testing contributes to the monitoring of individual patient health. It can also engage patients and motivate them to take an active role in managing their own health. Patient engagement is particularly important for managing high-risk patients, as shown in Medicare physician group practice (PGP) demonstration projects, precursors of ACOs. Many PGP project participants that achieved savings deployed strategies to encourage chronically ill patients to be more active in managing their own health.20
Laboratories can help engage patients by sharing laboratory results with patients directly. Test results can be accompanied by information that helps patients understand the implications of the results. This information can be valuable for patients as they discuss test results with treating physicians and determine if action needs to be taken.
Laboratory data can also be used to monitor the health status of a population. For instance, new coding systems (eg, LOINC and ICD-10) include laboratory data, such as HbA1c levels. Such data helps generate scorecards that indicate health status changes for individual patients as well as for populations.21 These scorecards can be used for risk stratification and for case managers and care coordinators to develop care management plans.
DATA ANALYTICS IS THE KEY
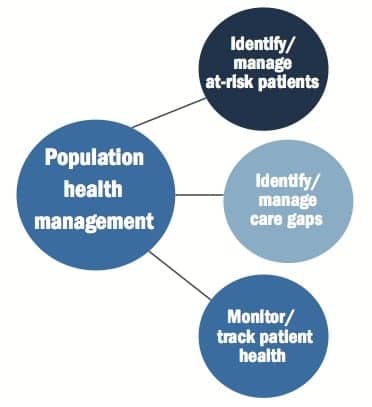
Figure 2. Population health management core activities for ACO laboratories. Source: Velusamy SR. Analytics: the key ingredient for the success of ACOs. HTC Global Services Inc. Available at: himss.files.cms-plus.com/FileDownloads/HTC%20ACO%20Analytics.pdf.
According to the Health Catalyst Q3 2014 survey among senior IT executives in healthcare, more than half (54%) predicted that analytics would be the next major HIT investment following the rollout of EHRs.22 Population health initiatives were ranked third in priority, selected by 42% of the respondents. Population health initiatives, however, were cited as the key driver of the demand for analytics by 84% of the respondents. Other drivers included quality improvement initiatives (79%) and accountable care or shared risk initiatives (68%). Nearly three-quarters of the respondents reported that analytics will be extremely important in their organizations in the near future.
Many ACOs are approaching population health management as a two-phase implementation. Many are targeting the most expensive patients, such as those with multiple chronic conditions, and working to improve care coordination for them in the initial phase. With the transition to the second phase, often referred to as “population health 2.0,” more ACOs will apply predictive analytics to a broader range of patients to proactively identify those in need of care.4
One ACO at the leading edge is the Geisinger Health System. Geisinger plans to use predictive analytics to manage care gaps among its patient population, with a focus on optimizing outpatient visits. For instance, patients with diabetes will be referred for laboratory testing before coming in for a visit so that the physician and the patient can review the results and plan next steps in a single visit. Other applications include efforts to assess patient risk for serious illness such as lung cancer, and recommend appropriate screening for high-risk patients.23 This system will help streamline care as well as improve patient engagement.
By fulfilling the data analytics need of ACOs, laboratories have an opportunity to demonstrate the value of laboratory services to population health management, quality improvement, and other accountable care initiatives. According to G2 Intelligence interviews, ACO laboratories currently have limited involvement with data analytics. A separate data analytics team typically handles this task, though laboratories provide input, when needed. This may change as ACOs progress. (For more information, see the companion article, “Laboratories Guide Data Analytics.”)
One reason why laboratories have not fully explored their potential in data analytics is lack of expertise in this area. Some ACO laboratories are approaching third party vendors to boost their analytics capabilities. G2 Intelligence surveys found that 18.5% of laboratories in ACOs have contracted with vendors for additional services, especially services related to data analytics, to support ACO performance. This engagement is more prevalent in experienced, older ACOs than in younger ACOs, possibly because of the greater needs for analytics support as ACOs mature.
Large independent laboratories have been actively pursuing ACOs to get involved in population health management. As margins for performing laboratory tests are diminishing with decreasing reimbursement, these laboratories view involvement in population health management as a new opportunity for business growth. (For more information, see the companion article, “Independent Laboratories Invest in Analytics to Support Population Health Management.”)
ACO laboratories, however, are lagging a bit behind. Some ACO laboratories are providing laboratory data, but are not involved in the actual analytics. Others are not taking part at all. “Our ACO has worked on primary care physicians (PCPs) and is now focusing on pharmacy,” a pathology director from a large hospital ACO said. “The next item on the list is radiology, and then there is lab. It will probably take another a year to get to the lab. So we are kind of hanging around waiting for them to start paying attention.”
LABORATORY INITIATIVES IN POPULATION HEALTH MANAGEMENT

Figure 3. ACO laboratory initiatives in population management. “Other” includes community outreach services. Source: G2 Intelligence.
According to G2 Intelligence surveys, ACO laboratories have several initiatives underway to support population health management (see Figure 3). Over half of laboratories (56.3%) are assisting ACOs in developing population health management standards. About half (50.7%) are integrating laboratory data or helping ACOs identify high-risk patients. Nearly one-third (31.0%) are including peer comparisons to aid the management of patients with chronic diseases and detection of patients with high-expense diseases such as cancer. Just 18.3% are employing pattern recognition, risk factor identification, and other clinical judgments and utilization observations in their analytics.
Although some ACO laboratories have a great head start in supporting population health management, there is ample room for improvement as ACOs move forward. As ACOs evolve, HIT matures, and data analytics advances, laboratories should constantly look out for new opportunities to get involved in population health management given its strategic importance in ACOs.
RECOMMENDATIONS FOR ACTION
Industry experts interviewed by G2 Intelligence generally believe that ACOs will continue to grow in counts, covered lives, and reach. To become value-added service providers and key participants in ACOs, laboratories should consider the following recommendations:
- Engage more actively in value initiatives across the care continuum.
- Develop metrics to quantify laboratory value contribution.
- Be proactive in approaching ACOs and get a seat at the table early.
Laboratory engagement in value initiatives varies across ACOs. Many laboratories have launched value initiatives, but few have achieved the level of visibility as desired in ACOs. Laboratory initiatives should shift the focus from operational efficiencies to clinical effectiveness by including efforts directed at providing stronger clinical decision support across physician populations, including primary care physicians (PCPs) that have traditionally had little interaction with laboratory professionals, and enhancing analytics support for population health management.
Along with the shift toward effectiveness-driven initiatives targeted at direct patient care, laboratories must develop metrics to capture the true value of laboratory services in ACOs in terms of system-wide contribution to cost savings and improving patient outcomes and population health. These metrics will help quantify the value contribution made by laboratories and prompt the ACO management to reconsider laboratory’s eligibility for shared savings and allocate proper financial compensation for laboratory contribution.
Although laboratories are not the centerpiece in initial phases of ACOs, it does not mean they should take a “wait-and-see” approach. Rather, laboratories should be proactive and engage in ACO discussions early. G2 Intelligence interviews found that many ACO executives are preoccupied with PCPs and high-risk patient management and have not devoted time and resources to explore the potential value of laboratory services, especially in areas of direct patient care, population health management, and system-wide cost savings.
Laboratories should be proactive in educating ACOs about the value of laboratory services. Pathologists, often viewed as specialists in many ACOs, should take the lead and step out of their comfort zone and collaborate with “physician champions” to promote the value of laboratory services. Other non-pathologist laboratory professionals will follow.
Jenny Xu, PhD, is a healthcare market research analyst and author of the G2 Intelligence report Laboratory Services in Accountable Care Organizations. For further information, contactG2 Intelligence customer service at (888) 729-2315..
REFERENCES
- This article contains excerpts from the research report Laboratory Services in Accountable Care Organizations, published by G2 Intelligence and is reprinted here with permission. All rights reserved © 2014 Plain Language Media. To obtain a full copy of this report, please call G2 Intelligence customer service at (888) 729-2315 or visit www.g2intelligence.com.
- Gamble M, Punke H. ACO manifesto: 50 things to know about accountable care organizations. Becker’s Hospital Review. September 3, 2013.
- Pantanowitz L, Henricks WH, Beckwith BA. Medical laboratory informatics. Clinical Laboratory Medicine. 2007;27(4):823–843.
- Evans M. Data collection could stump next phase of predictive analytics. Modern Healthcare. July 14, 2014.
- Larkin H. Population health: the risks and rewards. Hospitals and Health Networks. February 11, 2014.
- Moving from volume to value: participate at your own risk [white paper]. Covisint Corp. 2014.
- Velusamy SR. Analytics: the key ingredient for the success of ACOs. HTC Global Services Inc. Available at: himss.files.cms-plus.com/FileDownloads/HTC%20ACO%20Analytics.pdf.
- Agency for Healthcare Research and Quality: Cost fact sheet. US Department of Health and Human Services.
- Centers for Disease Control and Prevention. Chronic diseases at a glance. 2009.
- Zigmond J. Bill would encourage team-based care for medicare’s chronically ill. Modern Healthcare. January 15, 2014.
- Berardo J. The new face of chronic care management. MagnaCare. 2012.
- Anderson G. Key to healthcare costs is to better treat chronically ill. US News and World Report. July 18, 2011.
- Sbrana F, Cocci F, Papa A, et al. Routine laboratory tests to risk-stratify patients with chronic coronary artery disease. Journal of Cardiology. 2013;61(2):132–137.
- Amir O, Liu A, and Change ALS. Stratification of highest-risk patients with chronic skin ulcers in a Stanford retrospective cohort includes diabetes, need for systemic antibiotics, and albumin levels. Ulcers. 2012;Article ID 767861, 7 pages; doi: 10.1155/2012/767861.
- Chen P. Business of pathology: pathologists’ roles in the emerging healthcare delivery models [presentation]. Practical Advances in Pathology. January 30, 2011.
- Kravitz JK. Reforming the healthcare delivery system [presentation]. Geisinger Health System. 2012.
- Collaborative accountable care: Cigna’s approach to accountable care organizations [white paper]. Cigna. 2011.
- Marino DJ. How to translate ACO quality measures into clinical processes. Health Directions. 2014.
- Kaelber D, Kramer A. How to use technology to create value [presentation]. Better Health Greater Cleveland. Quality Improvement Learning Collaborative Summit XIV. April 11, 2014.
- Evans M. Medicare ACOs can learn lessons from earlier demo project. Modern Healthcare. August 26, 2014.
- Stricker P. Using data stratification and predictive modeling to support the case management process. CMSA.
- Analytics outweighs accountable care, population health, ICD-10 as an IT priority. Health Catalyst. September 11, 2014.
- Rodak S. Learning from the best: what HIM looks like at Geisinger, Intermountain. Becker’s Health IT and CIO Review. September 4, 2013.



{kind=link}