
New tests track unwanted responses of the immune system
By Craig C. Foreback, PhD
The wide varieties of human allergies are distinguished from one another by their assignment to one of four classes of hypersensitivity. Each of the classes of hypersensitivity defines different forms of harmful immune responses that an individual may have to inherently harmless environmental antigens such as drugs, foods, or pollens.
Most common allergies are classified as type I hypersensitivity responses, mediated by immunoglobulin E (IgE) antibodies after reexposure to a previously encountered allergen. However, allergic reactions to some drugs, such as penicillin, are classified as type II hypersensitivity responses, and are mediated by immunoglobulin G (IgG) antibodies.
It is estimated that roughly one in six Americans—about 50 million people—suffer from some type of allergy, including drug, eye, food, indoor/outdoor, insect, latex, and skin allergies. In the United States, allergies resulting from type I, IgE-mediated hypersensitivity have a high prevalence. Of particular concern are food allergies.
Allergies are no less troublesome on the global stage. Worldwide, it is estimated that 30% to 40% of the global population is affected by allergies.1 In industrialized nations, the prevalence of allergies has doubled in the past 10 to 15 years, with consequences ranging from being merely a nuisance to being life threatening.
The term “autoimmune disease” describes a group of illnesses in which the body’s immune system becomes misdirected and attacks the organs it was meant to protect. This mechanism is believed to be the underlying cause of as many as 100 serious, chronic illnesses that can affect almost every human organ system, including the endocrine, gastrointestinal, and nervous systems. Various autoimmune diseases can affect an individual’s blood, blood vessels, connective tissues, eyes, and skin. In the United States, 50 million people are living with some form of autoimmune disease. Women are disproportionately affected, leading the National Institutes of Health to name autoimmunity as a major women’s health issue.2
ALLERGIC REACTIONS
A type I hypersensitivity response doesn’t usually happen the first time an exposure to an allergen occurs. The IgE-mediated mechanism requires prior exposure to an environmental allergen in order to prime the body’s response. When reexposure to the allergen does occur, the body tends to mount exaggerated IgE-mediated responses that can vary widely in intensity. Some of these responses can be life threatening.
Allergens that prime the body’s response mechanisms encompass a wide variety of environmental factors, including drugs, dust, food, insect bites and stings, mold, pets, pollution—and even cockroaches. While allergic responses can occur at any time, they are most often triggered by reexposures involving dietary changes, infectious diseases, pollution, or a higher than usual level of a previously encountered allergen. Diesel exhaust, for example, can increase IgE levels 20- to 50-fold. Reactivity to cigarette smoke and sulfur dioxide can also be a problem for sensitive individuals.
Complex allergies are increasing among women. After puberty, more women than men suffer from allergies. The prevalence of asthma is consistently higher among women.
Insects. An insect sting typically results in pain, swelling, and redness confined to the sting site. But a sting can affect parts of the body remote from where it occurred.
Allergic reactions to stings can occur at any age, and even after many previous normal reactions to stings. It has been estimated that potentially life-threatening allergic reactions to insect venom occur in 0.4% to 0.8% of children, and 3% of adults. In the United States, insect sting reactions account for at least 40 deaths each year.
The majority of insect stings in the United States come from bees, hornets, wasps, and yellow jackets. However, red or black imported fire ants now infest more than 260 million acres in the southern United States, where they have become a significant health hazard. In the southeastern United States, these fire ants may be the number one agent of insect stings. There are fire ant species that are native to the United States, but the species that are currently causing the greatest health concerns are those accidentally imported to the United States from South America.
Molds. Outdoor molds can grow on rotting logs and fallen leaves, in compost piles, and on grasses and grains. Unlike pollens, molds do not die with the first frost in late fall or early winter; instead, they just stop growing during this time. In the spring, they grow on plants killed by the cold. Indoor molds grow in places where there is moisture, such as the kitchen, bathroom, and basement.

Louise Loughran, Siemens Healthcare Diagnostics.
Foods. “Currently, food allergens are commanding more attention than other allergens,” says Louise Loughran, global marketing manager for allergy, autoimmune, and metabolic assays at Siemens Healthcare Diagnostics, Tarrytown, NY. Most food allergies appear in early childhood, but they can develop at any age. Symptoms of a food allergy can range from mild to severe, including anaphylaxis.
While any food can cause an adverse reaction, eight types of food account for about 90% of all allergic reactions: eggs, fish, milk, peanuts, shellfish, soy, tree nuts, and wheat. Certain seeds, including mustard and sesame seeds, are also common food allergy triggers and are considered a major allergen in some countries. Once a food allergy is diagnosed, the most effective treatment is to avoid the food.
Among children, the foods most associated with food allergies are eggs, milk, and peanuts. Children may outgrow their allergic reactions to eggs and milk. Peanut and tree nut allergies are likely to persist.
Among adults, the most common food allergens are fish and shellfish, fruit and vegetable pollen (oral allergy syndrome), peanuts, and tree nuts. People allergic to a specific food may also experience an adverse reaction to related foods. A person allergic to one species of tree nut may be cross-reactive to others. Those allergic to shrimp may react to crab and lobster. Someone allergic to peanuts may have problems with tree nuts, such as pecans, walnuts, almonds, and cashews, and in very rare circumstances may have problems with other legumes.
Trees and plants. Pollen from trees can cause allergic reactions, particularly eye irritation. Pine needles often cause allergic reactions. Like other pollen-bearing plants, marijuana is an allergen that can cause allergic responses. A recent article summarizes research on the ways in which cannabis can act as an allergen.3
DIAGNOSING ALLERGIES
After taking a history, an allergist may order skin-prick tests or blood tests, which can indicate whether allergen-specific IgE antibodies are present. Skin-prick tests can provide results in about 20 minutes.4 A liquid containing a tiny amount of the allergen is placed on the skin of a patient’s arm or back. The skin is pricked with a small, sterile probe, allowing the liquid to seep under the skin. The test is considered positive if a wheal (resembling the bump from a mosquito bite) develops at the site where the suspected allergen was placed. As a control, the test uses a skin-prick with a liquid that doesn’t contain the allergen and should not provoke a reaction, allowing a comparison between the two test sites.

Jim Aguanno, PhD, Siemens Healthcare Diagnostics.
Blood tests measure the amount of IgE antibody to the specific allergen being tested. Results are typically available within 24 hours. In the United States, Siemens and Thermo Fisher Scientific (Phadia) are the major players for allergy blood testing. Both companies offer complete automation.
“Although skin-prick tests are still preferred by many allergists in the United States, the opposite is true in Europe, where blood testing is favored,” says Jim Aguanno, PhD, senior clinical specialist at Siemens Healthcare Diagnostics. “Blood testing for allergens is equivalent to skin tests.”

The Immulite 2000 and 2000 XPi immunoassay systems by Siemens Healthcare Diagnostics are automated random-access analyzers that perform a wide range of allergy and autoimmune disease tests.
For its Immulite 2000 immunoassay system, Siemens offers an expanding menu of specific allergens and allergen panels, including animals, dust mites, food, grasses, insects, medicines, molds, parasites, trees, and weeds. “Results can be obtained in 65 minutes, and most laboratories will report the same day,” says Aguanno. The Immulite system also offers an extensive menu of other immunoassays, including cardiac, endocrine, hepatitis, therapeutic drug monitoring, and thyroid testing.
Clinicians have historically used whole-allergen (extract) skin- or serum-specific IgE tests to identify patients with IgE-mediated allergies. These tests offer strong sensitivity, but only average specificity. Recent advances have led to the development of serum-specific tests for the components of allergens, which significantly improve the specificity of testing.

Thermo Scientific Phadia offers instrumentation designed for allergy and autoimmune testing; here, the Phadia 1000.
In 2011, Thermo Fisher Scientific acquired Phadia (Uppsala, Sweden), a company that offers instrumentation designed for allergy and autoimmune testing and is on the leading edge in developing allergen component tests and test methods. “The ImmunoCap immuno solid-phase allergen chip (ISAC) is a miniaturized immunoassay platform, where allergens are immobilized in a microarray,” says Joseph E. Jones, senior medical liaison for immunodiagnostics at Thermo Fisher Scientific Phadia US Inc, Portage, Mich. “The initial chip contained 23 allergens; since then, it has been continually improved by providing a larger number of allergens. In 2011, the ISAC 112 chip was made commercially available, offering 112 components from 51 allergenic sources such as common food and inhalant allergens.” ImmunoCAP assays can be performed on hundreds of allergens, such as animal dander, food, mold, pollens, common ragweed, and trees.
The ImmunoCAP test procedure, including all washing and incubation steps, can be performed in less than 4 hours. As an add-on, the company also offers ISAC Xplain software, which delivers evidence-based allergen information relevant to the individual patient.

The ImmunoCap immuno solid-phase allergen chip (ISAC), by Thermo Fisher Scientific Phadia, is a miniaturized immunoassay platform.
ImmunoCAP’s positive results are measured on a scale of arbitrary units called ISAC standard units (ISUs). The scale ranges from 0.3 to 100 ISUs. Test results are presented semiquantitatively in four classes corresponding to the level of allergen component-specific antibodies detected in the sample. In each class, higher IgE-specific levels correlate with increasing severity of allergy symptoms. ImmunoCAP test results can be used to detect sensitization to specific allergens and to help guide treatment decisions.

Joseph E. Jones, Thermo Fisher Scientific Phadia US.
In part because of the continually increasing prevalence of allergies worldwide, the use of blood testing to detect allergens is on the rise. Also favoring the use of blood testing are the ease of access to the method in many markets, and the growing availability of allergen component testing. “Most major reference laboratories are using ImmunoCAP assays for allergy testing,” says Jones.
AUTOIMMUNE DISEASES
It has been estimated that autoimmune diseases are responsible for more than $100 billion in direct healthcare costs annually.2 Taken together, autoimmune diseases affect women more than three times as often as they affect men (see Table 1), and they have been cited among the top 10 causes of death for women aged 65 and under. Autoimmune diseases have been reported as the fourth-largest cause of disabilities among women in the United States.

Table 1. Female to male ratios in autoimmune diseases. Source: American Autoimmune Related Diseases Association Inc.
Compared to men, women have enhanced immune systems that increase their resistance to many types of infections, but also make them more susceptible to autoimmune diseases. In the United States, 8% of the population suffers from autoimmune diseases, and 78% of those sufferers are women. Women are nine times more likely to develop lupus erythematosus than men.
Different ethnic groups are more susceptible to certain autoimmune diseases. African-American, Asian, Hispanic, and Native American women are two to three times more likely to develop lupus than Caucasian women—and at a much earlier age than previously thought.
Other autoimmune diseases include biliary cirrhosis, celiac disease, Crohn’s disease, Graves’ disease, Hashimoto’s thyroiditis, multiple sclerosis, rheumatoid arthritis, and vasculitis.
DIAGNOSIS OF AUTOIMMUNE DISEASES
Antinuclear antibodies (ANAs) are characteristic of many autoimmune connective tissue diseases. ANA assays have been available for 60 years, and they are used extensively for diagnosing and monitoring autoimmune diseases such as dermatomyositis, lupus erythematosus, polymyositis, scleroderma, and Sjögren’s syndrome.
Rivaling the service career of ANA assays, indirect immunofluorescence (IIF) microscopy has also played a significant role in laboratory medicine over the years. Although introduced more than 50 years ago, IIF microscopy remains the most widely used conventional technique for detecting ANAs.

Eric Hoy, PhD, Immuno Concepts.
“Immuno Concepts has been a major supplier of ANA slides containing HEp-2 cells for more than 20 years,” says Eric Hoy, PhD, chief scientific officer at Immuno Concepts, Sacramento, Calif. “IIF is the gold standard for ANA screening. However, it is time-consuming, labor-intensive, and requires highly trained personnel. It is also hard to standardize due to the subjectivity of interpretation. And the workload is increasing due to the aging population.”
To address these concerns, Immuno Concepts has developed an automated microscopy platform called the Image Navigator, which eliminates much of the time and labor required for IIF testing, while still allowing the laboratory professional to control the interpretation and reporting of the tests. The platform also integrates with the company’s AFT 2000 and AFT 3000 automated pipetting stations.
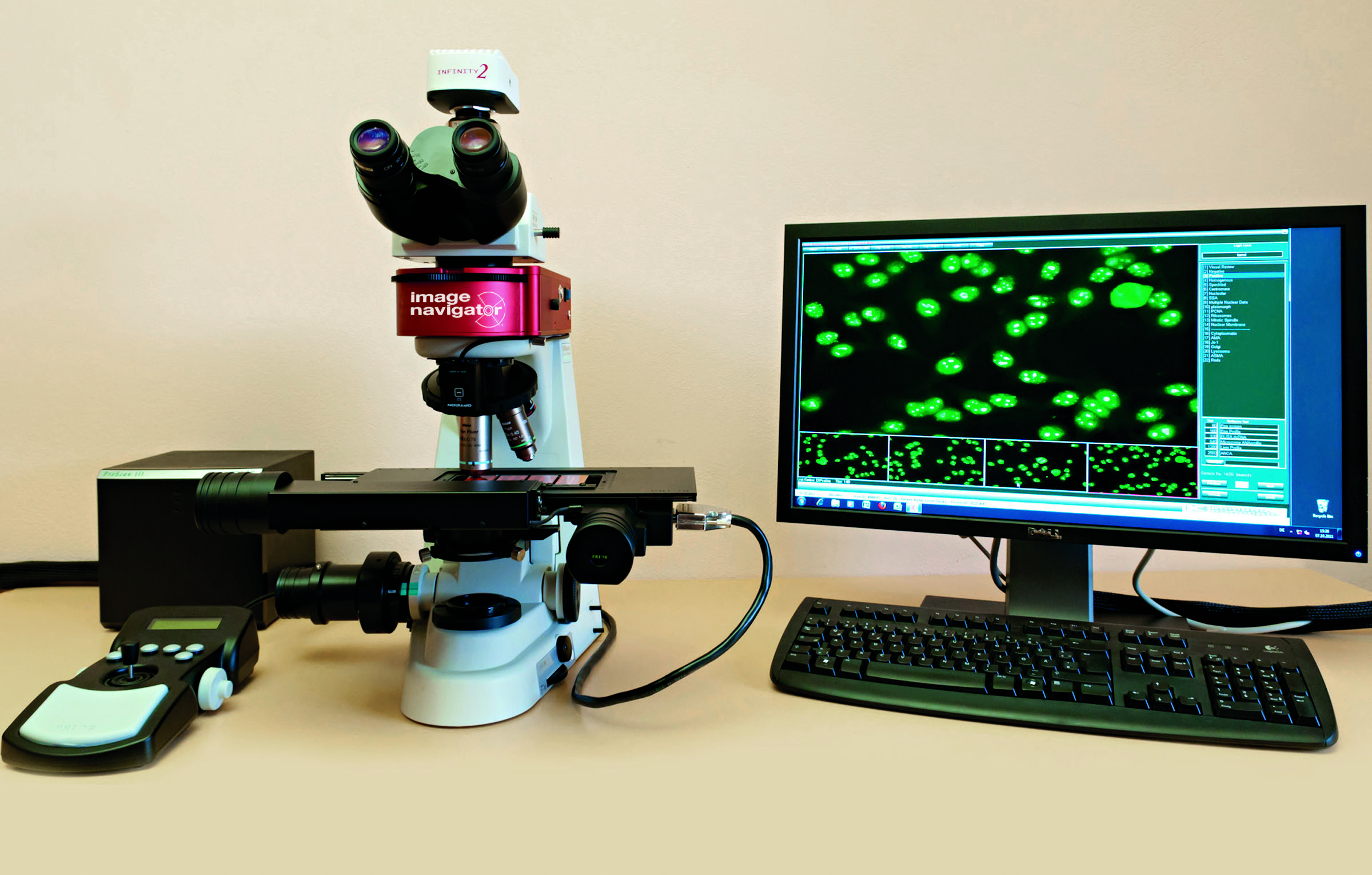
The Image Navigator by Immuno Concepts.
“The Image Navigator captures images of autoantibody IIF slides; separates the images into controls, possible positives, possible negatives, and titers; and presents these images to the laboratory professional on separate review screens for quick and easy confirmation and reporting,” says Hoy. “The system also includes a high-quality fluorescent microscope, so samples can be observed by the conventional method as well as in the automated format. All together, the system has been shown to significantly improve accuracy and reproducibility in the reading of IIF assays.” According to the company, FDA approval of the system is pending.
Multiplex Immunoassays. “Recent advances in protein classification methods have led to high-throughput multiplex immunoassays that allow simultaneous quantification of many analytes,” says Paulina Leung-Lee, senior sales product manager for Bio-Rad Laboratories Inc, Hercules, Calif. The company’s BioPlex 2200 multiplexing platform, based on fluorescent microbead technology, offers assays for a wide range of autoimmune diseases, including celiac disease, Crohn’s disease, lupus, rheumatoid arthritis, and vasculitis.

Paulina Leung-Lee, Bio-Rad Laboratories.
“The system’s ANA screen with medical decision support software performs qualitative screening of specific ANAs, including the quantitative detection of antibody to double-stranded DNA, and the semiquantitative detection of 10 individual antibodies (to chromatin, ribosomal-P protein, SS-A, SS-B, Sm, Sm/RNP, RNP, Scl-70, Jo-1, and centromere B) in human serum or plasma,” says Leung-Lee. The detection of these antibodies targets several connective tissue autoimmune diseases, including polymyositis, scleroderma, Sjögrens syndrome, systemic lupus erythematosus, and mixed connective tissue diseases. Evaluations of ANA measurement using the BioPlex instrument in multiple sites have been published.5,6
Tests for markers of celiac disease, rheumatoid arthritis, and systemic small vessel vasculitis are also available on the BioPlex system. Celiac disease is associated with human leukocyte antigen DQ8 and DQ2 genes. BioPlex assays for semiquantitative detection of IgA and IgG autoantibodies to deamidated gliadin peptide and tissue transglutaminase have been shown to offer excellent sensitivity and specificity for the detection of celiac disease.7

The Bio-Rad BioPlex 2200 multiplexing platform uses fluorescent microbead technology to perform tests for a wide range of autoimmune diseases.
The BioPlex system performs testing to detect anti-cyclic citrullinated peptide antibodies (anti-CCP), which is useful for the diagnosis of rheumatoid arthritis.8 The system’s anti-CCP test has been compared to an ELISA method.9 The study demonstrated that there was high concordance between the ELISA and BioPlex assays. The authors concluded that the BioPlex anti-CCP test is a powerful tool for the rapid assessment of anti-CCP and can replace ELISA methods.
The BioPlex system’s vasculitis reagent pack is a multiplexed test for the detection of IgG autoantibodies to myeloperoxidase, proteinase 3, and glomerular basement membrane—all of which are associated with systemic small vessel vasculitis.
Siemens has also obtained FDA clearance to offer US laboratories an anti-CCP IgG assay to aid in the diagnosis of rheumatoid arthritis. “Available on the company’s Immulite 2000/2000 XPi immunoassay systems, the anti-CCP IgG assay affords laboratories the ability to integrate testing for rheumatoid arthritis testing onto an automated, random-access analyzer,” says Loughran.
CONCLUSION
The incidence of allergies and autoimmune diseases has been increasing over the past several decades. Both diseases are a major women’s health issue.
New methods for diagnosis and treatment have become available, including automated analyzers from several market-leading IVD manufacturers. Adoption of testing with such advanced technologies will improve outcomes and reduce morbidity.
Craig C. Foreback, PhD, is a contributing writer and member of the CLP editorial advisory board. For further information, contact chief editor Steve Halasey via [email protected].
REFERENCES
- Pawankar R. Editorial: the unmet global health need of severe and complex allergies: meeting the challenge. World Allergy Organization Journal. 2012;5:20–21; doi: 10.1097/wox.0b013e31824a5552.
- Autoimmune disease in women. [online] Eastpointe, Mich: American Autoimmune Related Diseases Association Inc, 2015. Available at: www.aarda.org/autoimmune-information/autoimmune-disease-in-women. Accessed August 1, 2015.
- Ocampo TL, Rans TS. Cannabis sativa: the unconventional “weed” allergen. Ann Allergy Asthma Immunol. 2015;114(3):187–192; doi: 10.1016/j.anai.2015.01.004.
- Allergy testing: overview. [online] Arlington Heights, Ill: American College of Allergy, Asthma, and Immunology, 2015. Available at: http://acaai.org/allergies/treatment/allergy-testing. Accessed August 1, 2015.
- Sohn KY, Khan WI. ANA testing: from microscopy to multiplexing. Clin Lab News. 2014; 40(6):8–10.
- Moder KG, Wener MH, Weisman MH, et al. Measurement of antinuclear antibodies by multiplex immunoassay: a prospective, multicenter clinical evaluation. J Rheumatol, 2007;34(5):978–986.
- Holding S, Wilson F, Spradbery D. Clinical evaluation of the BioPlex 2200 celiac IgA and IgG kits: a novel multiplex screen incorporating an integral check for IgA deficiency. J Immunol Methods. 2014;405, 29–34; doi: 10.1016/j.jim.2014.01.002.
- Mouterde G, Lukas C, Goupille P, et al. Association of anticyclic citrullinated peptide antibodies and/or rheumatoid factor status and clinical presentation in early arthritis: results from the ESPOIR cohort. J Rheumatol. 2014;41(8):1614–1622; doi: 10.3899/jrheum.130884.
- Harich R, Roger C, Garnier L, Bienvenu J, Fabien N. Comparison of anti-CCP autoantibodies measurement by ELISA and a bead-based assay in a large patient cohort. Clin Biochem. 2014;47(6):485–488; doi: 10.1016/j.clinbiochem.2014.02.010.



{kind=link}