
Following best practices can help labs maximize the utility and cost-effectiveness of flu testing.
By Sheldon Campbell, MD, PhD, FCAP, and Norman Moore, PhD
Screening for influenza infection may be important for improving patient outcomes and reducing the public health impact of this potentially deadly illness. Yet, despite the availability of dozens of influenza testing devices, most such tests do not realize the full potential of diagnosis because they do not provide highly accurate results quickly enough for healthcare providers to make informed treatment decisions while the patient is still under their care.
The combination of suboptimal diagnosis, the highly transmissible nature of the virus, and the wide overlap of symptoms with more urgent conditions like pneumonia, has led to widespread empirical treatment, and sometimes overtreatment, of patients who present with influenza-like illness.

Sheldon Campbell, MD, PhD, FCAP, Yale School of Medicine.
There are many reasons that clinicians forego testing. Influenza appears on the differential diagnosis of many conditions affecting patients during the winter months, including upper respiratory, lower respiratory, and febrile syndromes. In addition, clinical guidelines from the US Centers for Disease Control and Prevention and other expert groups recommend initiating antiviral treatment within 48 hours of the onset of symptoms. In most cases, given the timing of patient presentation and the historical limitations of flu testing, such recommendations translate into empirical treatment. Unfortunately, studies have shown that evaluating patients for influenza based on clinical symptoms alone is inaccurate.1
This article will discuss the currently available influenza diagnostic methods with a focus on molecular testing—which has become the new gold standard for flu screening—and will provide guidance for selecting and utilizing influenza diagnostic tests. (For more information on current testing methodologies for influenza, access CLP’s free webcast “Influenza Testing Today: Keeping Up with a Moving Target.”)
GUIDING TREATMENT
Specific influenza diagnosis can empower healthcare providers to make more-effective decisions on hospital admission, antibiotic therapy, further diagnostic testing, and direct influenza therapies. Moreover, rapid diagnosis may help reduce hospitalizations, length of hospital stays, ancillary tests, and complications, thereby optimizing outcomes and reducing transmission of the virus.2–4

Norman Moore, PhD, Alere Inc.
Accurate, rapid diagnosis helps guide appropriate treatment decisions so that antibiotics can be withheld, and antivirals prescribed, as needed. In a retrospective analysis spanning three flu seasons, significantly more patients diagnosed without rapid influenza diagnostic tests (RIDTs) were given antibiotics compared with those who were diagnosed with rapid testing. Similarly, three times as many patients diagnosed with RIDTs received antivirals as those who were not diagnosed with RIDTs.
Despite such significant benefits, however, until recently influenza assays could not provide accurate results quickly enough for clinicians to make informed treatment decisions in an actionable timeframe.
IN USE TODAY
Today, a number of different types of influenza assays are widely used. The following paragraphs summarize the key methods represented by such commonly used assays.
Culture testing is often conducted in centralized labs. Long considered the gold standard for flu testing because of its high sensitivity and specificity, completion of culture testing requires around 4 to 5 days, limiting its impact on patient care. Newer “shell viral” (R-Mix) culture testing produces results in 48 to 72 hours.
Direct fluorescent antibody (DFA) tests produce accurate results in 1 to 2 hours and can be performed on specimen culture or directly on clinical specimens. However, the test is relatively complex to administer and requires additional reagents and equipment.
RIDTs that detect the presence of influenza virus antigens have become the standard means of diagnosing influenza virus. While this technology delivers results within 30 minutes with generally high specificity, rates of sensitivity range from poor to moderate across settings, populations, and tests. An analysis of flu tests used during the 2009 influenza A H1N1 outbreak in New York City showed that RIDTs identified that strain with sensitivity as low as 17.8%. However, a large-scale study demonstrated that flu testing with RIDTs among older adults led to appropriate treatment more often than no testing.2,5,6
Since their commercialization in the 1990s, polymerase chain reaction (PCR) and other amplified molecular tests have been widely adopted because they offer improved sensitivity. Amplified molecular tests are now the diagnostic gold standard for influenza virus detection. However, traditional PCR testing requires repeated and time-consuming thermocycling (temperature adjustments at each stage of DNA amplification), requiring complex instrumentation, delaying results, and limiting its utility for direct testing at the time of presentation.
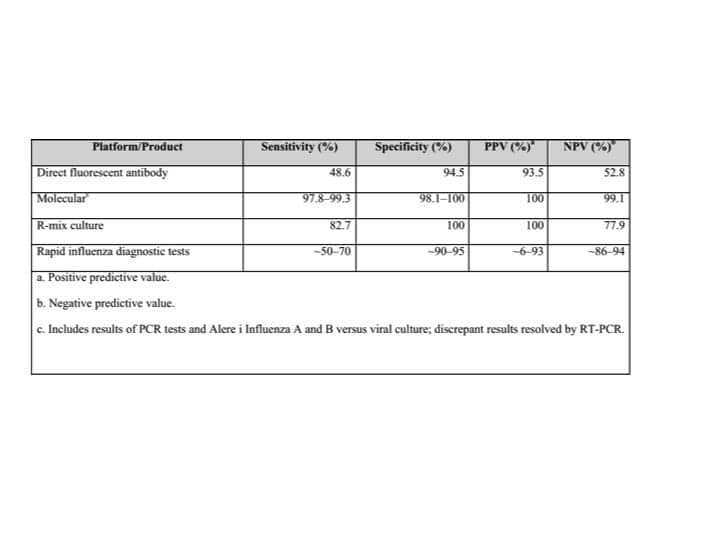
Table 1. Comparison of performance for diagnosing influenza among multiple classes of tests.5,8,9 Click to enlarge.
The strengths and limitations of these tests reflect the trade-offs between accuracy and speed that clinicians have traditionally had to make when selecting a diagnostic assay for their practice (see Table 1).
TEST EVOLUTION
Fortunately, testing platforms have evolved significantly in recent years. Today, molecular tests that offer lab-accurate results in an actionable timeframe—as quickly as 15 minutes—are transforming the detection and treatment of influenza. Detection properties vary from system to system, but as a class, molecular tests exceed culture in sensitivity, partly due to the susceptibility of culture methods to virus loss, corruption, or inactivation during transport. In addition, as molecular flu testing platforms are granted waived status under the terms of the Clinical Laboratory Improvement Amendments of 1988 (CLIA), healthcare providers can screen patients in a wide range of settings—increasing access to testing and streamlining care.
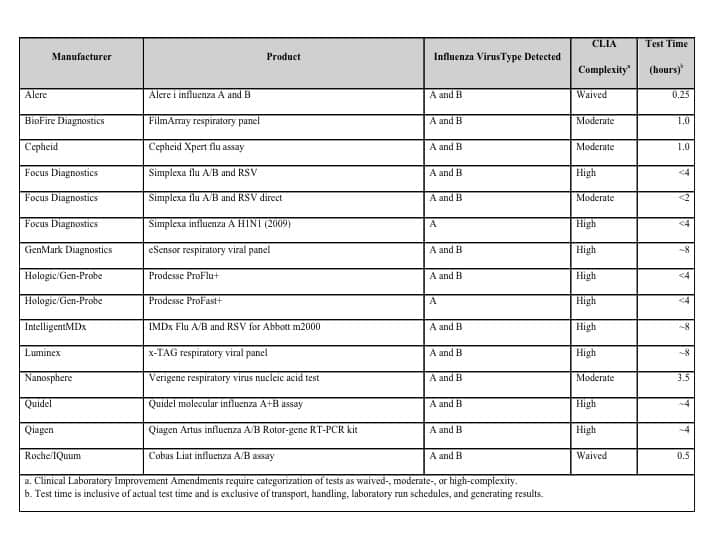
Table 2. Select FDA-cleared molecular flu tests.10 Click to enlarge.
The list of FDA-cleared molecular flu assays continues to grow (see Table 2). These products analyze nasopharyngeal or nasal swabs, span a wide range of time to results (from 15 minutes to 8 hours), and have varied CLIA complexity categorizations. Several of the cleared tests also detect other viral and bacterial illnesses.
Quantifying the cost-effectiveness of influenza screening is complicated by the wide range of variables at play, such as the inherently seasonal nature of flu testing, the duration and severity of a given flu season, the volume and multiple testing target capacity of tests, and utilization of antivirals. Even a large-scale study evaluating the cost-effectiveness of using rapid PCR flu tests among high-risk emergency department patients concluded only that the local prevalence of influenza at a given time had an enormous impact on cost-effectiveness. Similarly, parsing the cost of testing is difficult and requires accounting not only for the test itself but also for the reagent, instrumentation for sample extraction, and labor.7
BEST PRACTICES
The emergence of more-accurate, rapid, and easy-to-use molecular tests may eventually shift the cost-utility balance of flu testing. In the meantime, however, healthcare providers should adopt best practices to maximize the utility and cost-effectiveness of flu testing, regardless of the setting or the type of test deployed:
- Limit testing to high-risk patients and time periods. Testing should be offered only during flu season, or once influenza has been reported in your area. Administering flu tests off-season can affect their positive predictive value, which is based on prevalence. Office and hospital staff can use tools such as the CDC flu map to track the spread of viral activity. Exceptions to the general testing limitations may be made for occasional patients who have traveled to the southern hemisphere or the tropics, where influenza activity is different from that in the temperate northern hemisphere.
- Whenever possible, test early in illness. Flu tests are most sensitive early in illness, when patients are most infectious. Antiviral therapy for infected patients is most effective when initiated early.
- Train staff on correct specimen collection. Collecting nasopharyngeal samples is not difficult, but care must be taken to obtain ciliated epithelial cells, which are located almost by the front of the ear. A good collection is uncomfortable for the patient, but is essential for optimal testing.
- Select testing platforms that correspond to the needs and capabilities of the testing laboratory or setting. Platforms and assays that also detect other illnesses, such as respiratory syncytial virus (RSV) and Strep A, will have utility throughout the year. Economies of scale can make higher complexity tests have less labor per sample if done in high volume. No ‘one-size-fits-all’ solution is available; each facility should investigate the options and choose testing solutions to fit their situation.
Finally, despite recent advances in testing, prevention remains the cornerstone of influenza management. Healthcare professionals should take steps to prevent infection, such as getting vaccinated, paying attention to hand hygiene, and limiting contact with others when sick—and should encourage their patients to adopt these practices as well.
Sheldon Campbell, MD, PhD, FCAP, is an associate professor of laboratory medicine at the Yale School of Medicine; Norman Moore, PhD, is director of scientific affairs for infectious diseases at Alere Inc. For further information, contact CLP chief editor Steve Halasey via [email protected].
REFERENCES
- Monto AS, Gravenstein S, Elliott M, Colopy M, Schweinle J. Clinical signs and symptoms predicting influenza infection. Arch Intern Med. 2000;160(21):3243–3247.
- Blaschke AJ, Shapiro DJ, Pavia AT, et al. A national study of the impact of rapid influenza testing on clinical care in the emergency department. J Ped Infect Dis. 2014;3(2):112–118; doi: 10.1093/jpids/pit071. First published online November 13, 2013.
- Williams KM, Jackson MA, Hamilton M. Rapid diagnostic testing for URIs in children: impact on physician decisionmaking and cost. Infect Med. 2002;19(3):109–111.
- Bonner AB, Monroe KW, Talley LI, Klasner AE, Kimberlin DW. Impact of the rapid diagnosis of influenza on physician decisionmaking and patient management in the pediatric emergency department: results of a randomized, prospective, controlled trial. Pediatrics. 2003;112(2):363–367.
- Ginocchio CC, Zhang F, Manji R, et al. Evaluation of multiple test methods for the detection of the novel 2009 influenza A (H1N1) during the New York City outbreak. J Clin Virol. 2009;45(3):191–195; doi: 10.1016/j.jcv.2009.06.005.
- D’Heilly SJ, Janoff EN, Nichol P, Nichol KL. Rapid diagnosis of influenza infection in older adults: influence on clinical care in a routine clinical setting. J Clin Virol. 2008;42(2):124–128; doi: 10.1016/j.jcv.2007.12.014.
- Dugas AF, Coleman S, Gaydos CA, Rothman RE, Frick KD. Cost-utility of rapid polymerase chain reaction-based influenza testing for high-risk emergency department patients. Ann Emerg Med. 2013;62(1):80–88; doi: 10.1016/j.annemergmed.2013.01.005.
- Rapid diagnostic testing for influenza: information for clinical laboratory directors [online]. Atlanta: Centers for Disease Control and Prevention, 2015. Available at: www.cdc.gov/flu/professionals/diagnosis/rapidlab.htm. Accessed October 26, 2015.
- Alere i Influenza A and B [package insert 425-024]. Waltham, Mass: Alere, 2015. Available at: www.alere.com/us/en/support/doc-search.html. Accessed October 26, 2015.
- FDA-cleared RT-PCR assays and other molecular assays for influenza viruses [online]. Atlanta: Centers for Disease Control and Prevention, 2015. Available at: www.cdc.gov/flu/pdf/professionals/diagnosis/table1-molecular-assays.pdf. Accessed October 26, 2015.



{kind=link}
Why would testing during non-flu outbreak season skew the test results?
http://www.rapidxray.biz