
Amid competing technologies, flow cytometry makes a mark in clinical applications
By Steve Halasey
In the armamentarium of the healthcare community, flow cytometry has commonly been regarded as a tool best applied in research laboratories rather than in clinical laboratories. A workhorse technology that offers tremendous flexibility and power for detecting cellular abnormalities and identifying a wide range of pathogens, flow cytometry has nevertheless been mostly restricted to use in research settings, where studies contribute understandings that often find application through other diagnostic methods.

The FACSJazz cell sorter from BD Biosciences is a research use only instrument that facilitates a streamlined approach to single-cell sequencing. Photo courtesy BD Biosciences.
But in recent years, routine clinical applications of flow cytometry have begun to increase in number and complexity, driven largely by advances in the technology. In small steps originating with a number of different instrument manufacturers and reagent suppliers, clinical flow cytometry is benefitting from the availability of better reagents, increased attention to the automation of preanalytical processing steps, more colors to represent data points, more powerful lasers, better detectors, and extremely high-end informatics processing to deal with all of the data that the new instruments can generate. And by all accounts, there is much more technical elaboration still to come.
FLOW ADVANCES LEAD TO ROUTINE APPLICATIONS

Marc H. Meyers, MS, MBA, Meyers Consulting.
Flow cytometry has been used in life sciences research, particularly cellular biology, almost from the moment that the technology emerged from the Herzenberg Laboratory of Stanford University in the 1960s. “It has moved into the clinical diagnostic space, as a lot of technologies do, but in a lot of ways it has flown somewhat under the radar,” says Marc H. Meyers, principal of Meyers Consulting, San Francisco, a clinical diagnostics consultancy.
Unlike other technologies with diagnostic utility, such as clinical chemistry tests, enzyme immunoassays, or molecular diagnostics, explains Meyers, flow cytometry has been implemented primarily through the use of laboratory-developed tests (LDTs). “Flow cytometry is following the same path and format development as other technologies—from research applications to clinical applications and, in the clinical arena, from LDTs to commercial in vitro diagnostics (IVDs). But in many cases, clinical applications of the technology have not progressed beyond the LDT format. In part, this is due to the challenges of getting complex multivariate technologies through clinical trials. So instead, laboratories have taken up the slack and created clinical flow cytometry tests, which are developed, validated, and performed by flow cytometrists in clinical laboratories.”

Jeannine T. Holden, MD, MBA, Beckman Coulter Life Sciences.
Although clinical flow cytometry is dominated by LDTs, cytotemetrists aren’t entirely without help from IVD manufacturers. A handful of manufacturers have taken steps to move their instruments and reagents through review at FDA, and now offer agency-cleared instruments and tests for specific diseases. “Beckman Coulter’s emphasis on clinical flow cytometry means that we’ve got several FDA-cleared assays for routine tests with well-defined targets,” says Jeannine T. Holden, MD, MBA, director of scientific affairs for flow cytometry at Beckman Coulter Life Sciences, Miami, Fla. “These currently include lymphocyte subsets on both the FC500 and Navios cytometers, and stem cell enumeration on the FC500.”

Patty Sardina, The Binding Site.
With or without the assistance of extensive automation and standardized kits, flow cytometry has earned its place in clinical laboratories. “The clinical utility of flow cytometry is vast,” says Patty Sardina, senior product manager for reagents at the Binding Site, San Diego, “because you can get so much information from a single cell.” Key areas for the current use of clinical flow cytometry include those described in the following sections.
Immunodeficiencies. One of the earliest clinical applications for flow cytometry was developed during the 1980s, shortly after the human immunodeficiency virus (HIV) was first identified as the causative agent of acquired immunodeficiency syndrome, when labs began using the test to monitor patients’ CD4 T-helper cells. “As the CD4 count was more and more accepted as a standard clinical test, it became clear that decreases in that number correlated significantly with patients’ decreasing health and eventual death,” recounts Antony C. Bakke, PhD, D(ABMLI), technical director for flow cytometry at Clarient Diagnostic Services, a Neogenomics company, Aliso Viejo, Calif. “But since the advent of highly active antiretroviral therapy and other intensive therapies, it’s also been found that CD4 counts can normalize, indicating the therapy is having a positive effect.”
“In the past, CD4 monitoring was used to determine when antiretroviral therapy should be given to patients infected with HIV,” notes Sardina. “But now, the World Health Organization has changed its guidelines, and anyone who tests positive for HIV is automatically offered antiretroviral therapy. Flow cytometry testing of HIV patients’ CD3, CD4, and CD8 counts has been a big testing market for a long time. Nowadays, it’s regarded almost like low-complexity testing.”
Antony C. Bakke, PhD, D(ABMLI), Clarient Diagnostic Services.
Success in monitoring HIV gradually led to the use of flow cytometry for detecting other primary immunodeficiencies, which result from cell defects that can be detected and characterized by flow cytometry immunophenotyping. “There are quite a number of recognized immunodeficiencies now—over 250—and many of these can be detected by flow cytometry assays,” says Bakke. “Diseases such as chronic granulomatous disease, severe combined immunodeficiency, x-linked agammaglobulinemia, and some of the platelet deficiencies can be measured by flow cytometry. There are many standardized tests for immunodeficiencies that use flow cytometry.”
“Any time you need to characterize the phenotypic expression of cell surface proteins, flow cytometry is really the go-to technology,” adds Meyers.
Hematopoietic malignancies. Since flow cytometry first emerged from research settings, there has also been a huge expansion in the use of the technology to diagnose and stage patients with various forms of hematopoietic malignancy. “Leukemias and lymphomas are routinely detected by flow cytometry,” says Bakke. “This data is integrated with other information to arrive at a final diagnosis. Flow cytometry offers a very easy way to deal with specimens that are either liquid, like the leukemias, or semiliquid, like the lymph nodes involving lymphoma.”
“Flow cytometry is the most widely used diagnostic tool in the field of hematological oncology—particularly for leukemia and lymphoma,” agrees Meyers. “In conjunction with clinical presentation and empirical evidence, it is the primary tool used in the diagnosis of these diseases.”

Thomas S. Alexander, PhD, D(ABMLI), Summa Health System.
Significantly, most of the reagents used for flow cytometry testing of leukemia and lymphoma are classified by FDA as analyte-specific reagents (ASRs). “Companies used to package reagents together, so a lab could buy, for instance, a leukemia package,” says Thomas S. Alexander, PhD, D(ABMLI), an immunologist in the department of pathology and laboratory medicine for the Summa Health System, Akron, Ohio. “For a four-color application, the package would have four different vials of four colors each that could be used for leukemia typing. But FDA didn’t like that. Instead, the agency said an ASR should be one individual reagent.”
One result of that ruling was to increase the complexity of flow cytometry testing. “All of a sudden, four vials became 16 vials, sold as ASRs,” Alexander adds. “To use them, labs have to titrate them out, determine how much of each reagent should be used, what the storage conditions should be, and so on. It makes it a little bit more difficult to set up and perform the tests.”
On top of such complexity is that fact that some new markers survive adoption and use, while some do not. “A marker that was real hot about 5 years ago and faded very quickly is something called zeta-chain-associated protein kinase 70 (ZAP-70), which was used for some leukemia typing,” says Alexander. “It’s a very difficult marker to detect because it is present on cells at various levels. Some protocols picked it up well; some didn’t. At conferences, there were always sessions discussing different ways of detecting ZAP-70. Then, after 2 or 3 years, clinicians began to say, ‘This really isn’t telling us very much, so we don’t need it anymore.’ So, for a while, very few people were asking for ZAP-70. However, as the ZAP-70 protocols have become more standardized, clinicians have gained more confidence in the assay and have resumed ordering it.”
“Flow cytometry comes into play for many forms of hematological malignancy. It is commonly used to look at markers of disease progression, and to detect minimal residual disease among leukemia patients who may be in remission,” says Sardina. “Clonal abnormalities of cells, as seen in diseases such as paroxysmal nocturnal hemoglobinuria, is an area with low incidence. But flow cytometry lends itself well to testing for such diseases because of its sensitivity and ability to isolate and look at a small number of cells.”
“Of course for some cases molecular diagnostics are used, and they provide a different type of information,” says Bakke. “But the advantage of flow cytometry is that we don’t have to know a specific gene that’s been modified in order to detect disease. We can use other features that indicate an abnormal cell.”
At the Dana-Farber Cancer Institute, the flow cytometry core facility maintains two high-speed analyzers for sterile sorting and analysis of samples in support of cancer research. Photo: Sam Ogden/Dana-Farber Cancer Institute.
Transplantation applications. One routine application of clinical flow cytometry that has FDA approval is the analysis and enumeration of stem cells, which is performed when patients are being prepared to receive stem cell transplants. “Bone marrow transplants can be quite painful to the donor, so that procedure has now been almost completely replaced by peripheral stem cell transplants,” says Bakke. “Stimulating the patient with cytokines causes the release of stem cells that are normally in the bone marrow into the peripheral circulation. Once there, the stem cells can be tested and enumerated until the level peaks, at which point the stem cells are harvested and stored until they can be given to the recipient.”
Flow cytometry is also used in applications where cell sorting—that is, physical separation—is performed in conjunction with stem cell transplantation. “After a transplant, patients have the best response when a chimera is formed. In that case, the patient has some of their own white blood cells coexisting with white blood cells from the donor,” says Bakke. “That type of chimera is the most effective at killing tumor cells.
“To determine if a posttransplantation chimera has formed, flow cytometry is used to sort some white blood cells from the patient. Then the separated cell populations are examined genetically to determine the percentage from the donor and from the recipient.”
“Flow cytometry is big in both pre- and posttransplantation testing,” says Sardina. “It is used for T-cell crossmatching to make sure there are no graft-versus-host mismatches, and it is used in postoperative monitoring to detect early transplant rejection and the effectiveness of any immunosuppressants that may be in use.”
Fetal-maternal hemoglobin monitoring. Another FDA-approved application for flow cytometry is monitoring fetal-maternal hemorrhage, which involves detecting fetal red blood cells in the maternal circulation in cases of injury or trauma. When a woman is pregnant, there can be problems if the woman suffers an injury. Correspondingly, the fetus may also be injured, potentially bleeding some of its own red blood cells, which contain fetal hemoglobin, into the mother’s circulation. Such instances can be monitored using flow cytometry.
“A small blood sample is taken from the mother, and is then assayed to determine if fetal cells are present,” says Bakke. “If so, that indicates there was a bleed. If the problem is significant enough, the physician may treat the fetus by providing a transfusion or, if the fetus is mature enough, by inducing delivery.”
In many cases, flow cytometry is selected for this purpose over other diagnostic methods. “Flow cytometry is useful when looking at fetal-maternal hemorrhaging and Rh-factor problems because it is so much more sensitive than conventional methods,” says Sardina. “It is able to provide much more sensitive data, so that physicians can look at treatment options in a much better way.”
Autoimmune disorders. Flow cytometry also has proven utility for the detection of autoantibodies that may signal the presence of such autoimmune disorders as ankylosing spondylitis, anterior uveitis, or reactive arthritis. In relation to such conditions, says Sardina, “testing for human leukocyte antigen B-27 has been on the rise in the marketplace.”
OBSTACLES TO ADOPTION
In spite of the broad utility of clinical flow cytometry, a number of factors may be hindering the development and adoption of additional tests using the method.
One such obstacle is the fact that flow cytometry tests are almost all categorized as high-complexity assays under the requirements of the Clinical Laboratory Improvement Amendments of 1988, so performing them typically requires staffing by doctoral-level scientists. “Most of this testing is run in the hands of very highly trained staff,” says Meyers. “Sometimes those who are designing these tests or adopting the tests from their colleagues are MD-PhDs. Flow cytometry tests can be difficult to develop, difficult to validate, and difficult to run.”
“Flow cytometry testing is not a black box,” agrees Bakke. “Labs need somebody who is trained and knows what they’re doing. The average medical technologist who has just finished school doesn’t have sufficient knowledge to handle one of these instruments. So performing flow cytometry tests leads to an issue of how to recruit and retain trained personnel.”
In addition, the tests are high complexity for good reason: in most cases, lab professionals have to create every reagent cocktail they use from scratch, using analyte-specific reagents, and there is a significant amount of preanalytical work to be done. “A hematopathologist who is setting up a test to obtain a diagnosis has to create the assay and test the panel of different conjugates that will be used in the analysis, and then validate the performance of the test,” says Meyers. “And then, if the hematopathologist is not going to be running the test personally, a team needs to be recruited and trained so that the test can be run in a perpetual manner. That’s a lot to ask.”
All of this preparation takes time, too. As much as 2 hours of preanalytical work may be needed before running a sample (which may take only 30 seconds). Such complexities also serve to increase costs and staffing requirements, which are a tough sale in a time when both money and highly trained people are hard to find.
Another major obstacle is the fact that flow cytometry tests tend to be fairly expensive in terms of the reagents, the amount of upkeep, and the routine quality control that is required. “For a hospital that only sees a handful of leukemia or lymphoma patients a day, it is probably cost prohibitive to set up one of these instruments,” says Bakke. “But a medical center that typically sees more than a dozen or 15 such patients a day may reach the point at which it can break even. At that point, it becomes worthwhile to find a well-trained individual. Fortunately, there are organizations that offer training courses specifically for clinical flow cytometry.”
ADVANCING TECHNOLOGY
Advances in flow cytometry technologies have been significant, leading to greater automation, higher performance, and an increased range of capabilities for clinical applications. “The technology has really exploded over the past 5 or 10 years, with a lot of new market entrants offering instrumentation, and a lot of new discoveries in reagents, fluorophores, and dyes,” says Sardina. “In the past, flow cytometry was so complex that it was associated with a lot of ease-of-use issues. But now it’s become much easier to use. The latest generations of instruments are finally catching up with technologies that have been available in other fields for many years, including the adoption of user-friendly software. And clinical applications of the technology are also growing along those lines.”
“On the hardware side, the first instrument we had would do three colors, representing three different parameters on cells,” says Alexander. “We’re looking now to acquire a new instrument that will have 10 colors, allowing us to look at 10 different parameters on each cell. That reduces the number of tubes that we need to run through and also gives us more information per cell.”
“There are a lot of new developments in the flow cytometry equipment that will be coming out in the near future,” says Bakke. “Right now, there are quite a few clinical labs that still use four- to six-color flow. But most of the advanced labs like mine have gone to 10-color, and some are up to 17- or 18-color. The ability to detect more fluorochromes, which correspond to more proteins on each cell, is one of the advances occurring right now.
“Being able to measure smaller and smaller particles—down to the size of nanometers—is also a capability that is becoming available,” Bakke adds. “It is not generally available right now, but there are new instruments coming that will provide that capability.”
Improvements in software have also contributed to simpler test processes, including postanalysis color compensation to the test parameters. “When a test involves a number of different fluorescent molecules, an analysis tube or region is set up for each color. And although each one is run individually, there’s always a little bleed,” says Alexander. “We need to account for and compensate for that.
“Making that compensation used to be an extremely complex procedure and had to be done before the specimen was run through. We had to kind of guess what it was going to be,” he adds. “Now we run controls that automatically set up the test parameters, and if additional compensation is needed, it can be very easily accomplished during postanalysis. To change the parameters of a region, all we have to do is click and drag it onscreen. Improvements such as these have made postanalysis and follow-up a lot simpler than they used to be.”
“Clinical instruments also now have fixed optical systems, where the flow cell is fused to the lens where the laser comes through,” says Alexander. “It used to be that was very fluid, and required adjustment each time the instrument was run to make sure the flow cell was properly lined up. Research instruments are still set up that way, because such an adjustment can be used to increase the sensitivity of the machine. But making that adjustment all the time was very difficult, and for clinical instruments it isn’t necessary. Clinical labs don’t have time to play around with such settings, so they just want it fixed.”
Clarient’s Antony C. Bakke, PhD, D(ABMLI) with a 10-color Beckman Coulter Navios flow cytometer. Photo: Clarient Diagnostic Services.
In the past decade, there have been a lot of improvements in the reagents available for clinical applications. “Getting standardized reagents—and having them be high-quality reagents—has been a big improvement,” says Bakke. “But there’s still some way to go.
“Right now, under FDA regulations, reagent suppliers can’t sell mixtures of reagents to labs; they can only sell individually packaged ASRs. As a result, each lab has to qualify and titrate each reagent individually to determine the right amount to be used. Performing a 10-color assay, for example, requires that 10 individual reagents be characterized, standardized, and mixed into a specific formula.”
While flow cytometry testing has already benefitted from significant improvements in specimen processing and standardized instrument calibration, further improvements in automation are also on the horizon. “There will be more automatic processing to take specimens all the way through a standardized process,” says Bakke. “Already, labs that have high throughput are trying to standardize as many of these steps as possible.
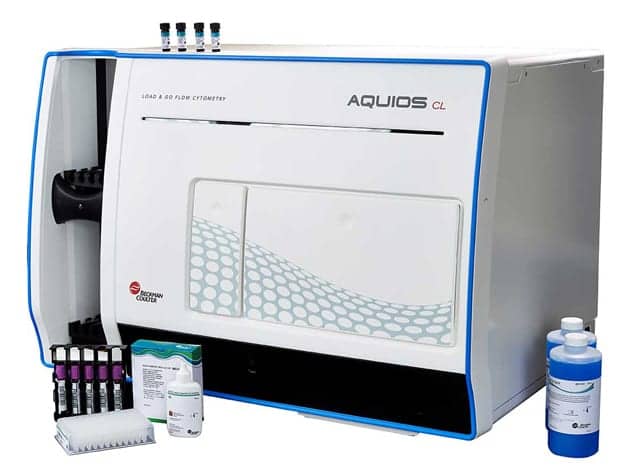
Beckman Coulter’s newest FDA-cleared platform is the Aquios CL, a load-and-go flow cytometer. Photo courtesy Beckman Coulter Life Sciences.
An example of improved automation is Beckman Coulter’s newest FDA-cleared platform, Aquios. “Aquios combines data acquisition, analysis, and fully automated sample preparation with dedicated bar-coded reagents and bidirectional laboratory information system connectivity,” says Holden. “Aquios’s workflow improvements translate to 24/7 availability for lymphocyte subsets, while permitting labs to turn their attention to complex LDTs.”
A good improvement in the near term will be the achievement of greater standardization across laboratories. “In Europe there is a program called Euroflow, for which several dozen laboratories have standard operating procedures, so that all of the labs produce comparable data even if they have different instruments,” adds Bakke. “In the United States, achieving such coordination will be a little bit more difficult. We don’t yet have that level of standardization among laboratories.”
EXPANDING UTILITY
New areas of clinical application include detection of blood-borne microparticles for the diagnosis of heart attack and stroke, measurement of molecular changes in cells, and detection of circulating tumor cells (liquid biopsies).
“A newer area that is developing involves monitoring some of the changes that occur during heart attacks and strokes,” says Bakke. “It turns out that those processes produce a lot of microparticles—very small vesicles that are released from platelets, from endothelial cells, and from white blood cells. Those microparticles can be measured and used to indicate what kind of an event has happened and how serious that event was. This application is quite new, so it’s not yet a type of testing that is being performed routinely.”
On the other end of the scale in terms of size, circulating tumor cells have recently captured the attention and imagination of many researchers, including those in IVD companies that hope to develop an early-detection alternative to surgical biopsies for both primary and metastatic cancers.
“Looking for circulating tumor cells is another application of flow cytometry,” says Bakke. “The really good labs can find one abnormal cell out of a million normal cells—that is, 10–6 sensitivity. And that becomes the goal for detecting tumor cells and also detecting minimal residual disease.
Tests for circulating tumor cells fall into two broad categories, Bakke explains. The first application is intended to detect and collect circulating tumor cells in order to determine what kind of tumor or metastases they represent. The second application is intended to quantitate the patient’s minimal residual disease, and comes into play after a patient’s solid tumor or hematopoietic malignancy has been treated.
Typically, the goal of cancer therapy is to kill off as many malignant cells as possible, and to reduce the number of tumor cells in peripheral blood to less than 1 in 10,000. “Detecting more than 1 tumor cell out of 10,000 normal cells indicates that the patient is much more likely to have a relapse; but if the treatment can push the number down to less than 1 out of 10,000 then the patient is less likely to have a relapse,” says Bakke. “There is a significant difference in the clinical response. Looking for that minimal residual disease is one increasing use of flow cytometry. It is being recommended by a number of international cancer agencies.”
CONCLUSION
While applications of clinical flow cytometry are increasing, it’s uncertain whether the technology will ever rival the major players that already dominate laboratory medicine. “The current situation of flow cytometry is similar to what happened in molecular diagnostics, and before that in clinical chemistry, where the methodologies were initially used in much more research-oriented applications, and then moved into the clinical phase and became IVD tests—but it took a while,” says Meyers. “For molecular diagnostics, that shift took place when the tests involved single-variable assays, or maybe double-variable assays—but not much more than that. Moving into much more complex multivariate analysis interrogation of a sample will probably take some time.”
In the meantime, flow cytometry is continuing to evolve in new directions with even greater utility for clinical testing. “In the not-too-distant future we are going to be fusing aspects of flow cytometry with molecular biology, which could become a very exciting area in terms of determining specific types of cancers and how they can be treated,” says Bakke. “I think there are still a lot of future applications and changes that are going to be happening.”
“There’s a ton of opportunity and utility,” agrees Sardina. “Because market advances are making flow cytometry simpler, smaller, and more affordable, more and more people will be using it. Over the next 5 to 15 years, we’re definitely going to see more assays and more novel ways to utilize it.”
Steve Halasey is chief editor of CLP.




{kind=link}
Nice Blog! Thanks for sharing this.