
New guidelines and advanced tests enable earlier diagnosis and improved patient outcomes
By Craig C. Foreback, PhD

Craig C. Foreback, PhD.
According to the US Centers for Disease Control and Prevention (CDC), “sepsis” is the body’s “overwhelming and life-threatening response to a bacterial or fungal infection, which can lead to tissue damage, organ failure, and death.”1 It is one of the most important causes of mortality in the United States, leading to nearly 260,000 deaths each year. It is also the nation’s most expensive hospital-treated condition, with costs to the healthcare system exceeding $20 billion each year and accounting for almost 7% of all Medicare costs.2
The concept of sepsis reflected in CDC’s summary definition has not always seemed so clear-cut. Ever since 1991, when a consensus conference first adopted clinical criteria for treating sepsis as a host response to infection—termed systemic inflammatory response syndrome (SIRS)—the medical profession has struggled to identify variables that would enable sepsis to be quickly recognized in everyday practice.3 A 2001 consensus conference sought to update the accepted definitions of “sepsis” and “septic shock,” but was unable to develop criteria that would be more precise.

Performed on BioFire’s FilmArray molecular testing platform, BioMérieux’s meningitis/encephalitis panel tests cerebrospinal fluid for the most common bacteria, viruses, and fungi responsible for community-acquired meningitis or encephalitis.
Since that time, however, considerable advances have been made toward understanding the epidemiology and pathobiology of sepsis—including changes in organ function, morphology, cell biology, biochemistry, immunology, and circulation—as well as its management. In January 2014, recognizing the need to reexamine existing definitions, the European Society of Intensive Care Medicine and the Society of Critical Care Medicine convened a task force of 19 critical care, infectious disease, pulmonary, and surgical specialists.4 The task force was charged with developing updated consensus definitions for “sepsis” and “septic shock.”
The newly revised definition of “sepsis” specifies that it is a life-threatening organ dysfunction caused by a dysregulated host response to infection. For clinical operationalization, organ dysfunction can be represented by an increase in the (sepsis-related) sequential organ failure assessment (SOFA) score of 2 points or more, which is associated with in-hospital mortality greater than 10%.
Meanwhile, based on a consensus process using results from a systematic review, surveys, and cohort studies, the task force recommended that “septic shock” be defined as a subset of sepsis in which particularly profound circulatory, cellular, and metabolic abnormalities are associated with a greater risk of mortality than with sepsis alone. Patients with septic shock can be clinically identified by hypotension requiring vasopressor therapy to maintain a mean arterial pressure of 65 mmHg or greater, and a serum lactate level greater than 2 mmol/L (>18mg/dL) after adequate fluid resuscitation.5,6
The combination of sepsis and septic shock is associated with hospital mortality rates greater than 40%. In out-of-hospital, emergency department, or general hospital ward settings, adult patients with suspected infection can be rapidly identified as being more likely to have poor outcomes typical of sepsis if they have at least two of the following clinical criteria that together constitute a new bedside clinical score termed quick SOFA (qSOFA):
- Respiratory rate of 22/min or greater
- Altered mental activity
- Systolic blood pressure of 100 mmHg or less
WHO CAN GET SEPSIS

Kevin Krenitsky, MD, OpGen.
“Anyone can get sepsis. However, patients with compromised immune systems are particularly at risk,” says Kevin Krenitsky, MD, president of OpGen, Gaithersburg, Md, a company that develops molecular diagnostics and offers testing services to combat life-threatening antibiotic-resistant infections. Other populations at risk include babies and young children; elderly people; people with chronic illnesses such as AIDS, cancer, diabetes, kidney disease, and liver disease; and people with severe burns or wounds.
Moreover, any type of infection, including candidemia and invasive candidiasis, can cause sepsis. “Staphylococcus aureus is a major cause of sepsis,” says Krenitsky.
S. aureus is the most common pathogen found in positive blood cultures among hospitalized patients. But species of coagulase-negative staphylococci (CoNS)—normally common and nonthreatening inhabitants of skin and mucous membranes—constitute another group of contaminants that are frequently encountered in association with nosocomial infections.
SEPSIS DIAGNOSIS
The original consensus definition for the diagnosis of sepsis, first published in 1992, was based on clinical signs and laboratory results that together make up systemic inflammatory response syndrome (SIRS).7 SIRS criteria included two or more of the following:
- Body temperature <36oC or >38oC
- Heart rate >90 beats per minute
- Respiratory rate >20 breaths per minute, or PaCO2 <32 mmHg
- White cell count >12/mL or >10% immature band forms
Sepsis was considered to be present when a patient met the SIRS criteria due to the presence of infection.

Using its benchtop Alere i isothermal nucleic acid amplification technology, Alere offers a wide variety of rapid infectious disease tests whose results are available in 15 minutes.
More recently, guidelines created by the Society of Critical Care Medicine’s Surviving Sepsis Campaign have emphasized the role of serum lactate as a criterion for septic shock. Lactic acid is an indicator of tissue ischemia; by the time that a patient’s lactic acid levels have begun to increase, sepsis has already begun to escalate. Although many institutions have not adopted a lactate level ?2 as part of the definition of end-organ dysfunction, the recently published guidelines clearly recommend that lactate levels be measured early on—within the first 3 hours of presentation—in order to identify patients with sepsis. Measuring a patient’s lactic acid concentration is currently part of the standard of care, and is included in the early goal-directed therapy guidelines as well as the bundled testing recommendations of the Surviving Sepsis Campaign.
Multiple studies have established that timely administration of appropriate antibiotics significantly reduces mortality due to severe sepsis and septic shock. Use of inappropriate empiric antibiotics is a common factor associated with mortality rates as high as 75%.8,9 Delays in initiating antimicrobial treatment are correlated with a progressive increase in mortality.10
At present, selection of initial antibiotics for the treatment of bacteremia must be determined empirically. Standard blood culture procedures currently consist of inoculating a blood culture bottle and placing it on an automated continuous monitoring and alert platform.11 Upon positivity, the contents are Gram stained, plated on appropriate media, and allowed to grow for 18 to 42 hours or longer, with subsequent subcultures and susceptibility testing as appropriate. The delay between collection of a blood sample from a patient and availability of traditional identification and susceptibility results has obvious implications for patient care.
Reducing the time required to obtain accurate identification and susceptibility results may lead to improved patient outcomes. Newer technologies such as nucleic acid amplification tests, fluorescence in situ hybridization (FISH), and matrix-assisted laser desorption ionization time-of-flight mass spectrometry (MALDI-TOF MS) provide rapid identification of pathogens and codetection of key resistance markers directly from positive blood cultures. The turnaround time from positive blood culture to results can be markedly reduced compared with traditional methods, potentially providing clinically useful data hours or days before traditional methods.
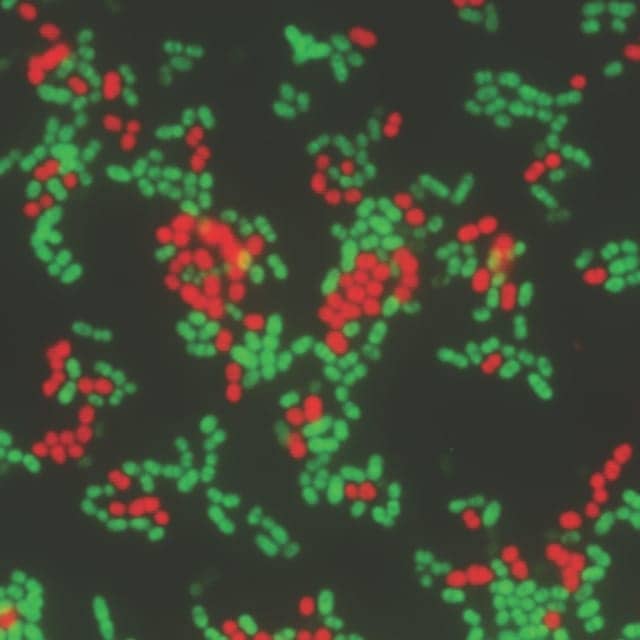
The Staphylococcus QuickFISH assay by AdvanDx can detect and differentiate Staphylococcus aureus from coagulase-negative staphylococci in 30 minutes.
AdvanDx, Woburn, Mass, a market leader in molecular testing of positive blood cultures, offers the Staphylococcus QuickFISH assay, which can detect and differentiate Staphylococcus aureus from coagulase-negative staphylococci (CoNS) in 30 minutes (see Figure 1). “Rapid identification and resistance reporting may allow deescalation of empiric coverage to appropriate targeted therapy and reduction in length of hospital stay,” says Krenitsky.
A recent study at Winter Haven Hospital, Winter Haven, Fla, illustrates the effectiveness of the QuickFISH assay.12 Initial results demonstrated an average reduction in length of stay of 2.28 days, an average reduction in vancomycin use by 0.5 days, and a projected savings to the hospital of $764,000 annually.

Wesley J. Candelaria, MPH, M(ASCP), Maricopa Medical Center.
Wesley J. Candelaria, MPH, M(ASCP), clinical laboratory director at Maricopa Medical Center/ Maricopa Integrated Health System implemented the QuickFISH test with remarkable results. “The Maricopa Medical Center is a county hospital with a high percentage of uninsured or underinsured patients,” says Candelaria. To contain costs, faster identification of Staphylococcus aureus bacteria was pursued. Quicker turnaround time led to reductions in length of stay, reductions in the use of antibiotics, better antibiotic targeting, and higher confidence in accurate identification, all together reducing the incidence of septicemia. “Length of stay was reduced by an average of 1.5 to 2 days,” says Candelaria. “Accompanied by significant reductions in antibiotic usage, yearly savings of $1.2 million have been achieved.”
Norman Moore, PhD, Alere.
Alere, Waltham, Mass, offers a wide variety of rapid infectious disease tests whose results are available in 15 minutes (see Figure 2). “Alere offers tests for HIV, influenza A and B, Legionnaires’ disease, MRSA, penicillin-binding protein 2a from Staphylococcus aureus isolates, pneumonia, and Staphylococcus aureus,” says Norman Moore, PhD, director of scientific affairs at Alere. All of these tests are essential for evaluating potential causes of sepsis. Because HIV in its early stages often mimics other infectious diseases, it must be ruled out. Sepsis is often a complication of Streptococcus and Legionella pneumonia.13 “The availability of rapid testing for a variety of infectious agents is an important tool for the physician in the fight against sepsis and containing the spread of infections in hospitals,” says Moore. “Rapid reporting assures a better result from the first phone call.”
CANDIDA AND SEPSIS
Few advances have occurred in the past decades to adequately address the most severe and costly infectious diseases affecting hospitalized patients, such as invasive fungal infections. Candida infections are increasing among hospitalized patients. “About 10% of sepsis patients suffer from Candida infections,” says Tom Lowery, PhD, chief scientific officer at T2 BioSystems, Lexington, Mass.

Tom Lowery, PhD, T2 BioSystems.
“Hospitalized patients with Candida infections have a 40% morality rate,” says Lowery. “Microbiologic cultures, the current gold standard diagnostic method for invasive Candida infections, have low specificity and can take 2 to 5 days to grow. T2 BioSystems’ T2MR technology is able to correctly characterize 98.1% of patients as noncandidemic, with a mean time to negative result of 4.2 hours” (see Figure 3).14
“The ability to rapidly and accurately exclude the possibility of candidemia can have significant implications in clinical practice,” says Lowery. “Decreasing the number of patients who need to be on empiric antifungal therapy, and thus decreasing the incidence of resistant strains, results in reduced potential for the side effects of antifungal treatment as well as substantially reduced healthcare costs.”
SEPSIS BIOMARKERS
The two most commonly used biomarkers for diagnosing infections that may lead to sepsis are C-reactive protein (CRP) and procalcitonin (PCT). CRP is not sufficiently specific for diagnosing sepsis, as it can also become elevated as a result of a number of other conditions, such as autoimmune disease, burns, cancer, cardiovascular disease, surgery, and trauma. PCT is a biomarker whose levels increase precipitously in patients with severe bacterial infection. It elevates prior to rises in lactic acid and is more specific for sepsis. Therefore, it is an important aid in the diagnosis of sepsis.

Sam Bozzette, MD, PhD, bioMérieux.
“Adding testing for PCT provides a much clearer clinical picture for diagnosing sepsis,” says Sam Bozzette, MD, PhD, vice president of medical affairs, Americas, and global health economics and outcomes research at bioMérieux. “Today, thousands of hospitalists and ED and ICU clinicians across the country use bioMérieux’s Vidas BRAHMS PCT assay to help them detect sepsis as soon as possible.” The Vidas PCT test generates results in 20 minutes, providing timely information to clinicians (see Figure 4).

The Vidas BRAHMS procalcitonin assay, performed on the benchtop Vidas multiparametric immunoassay analyzer by bioMérieux, generates results in 20 minutes, helping clinicians to detect sepsis as early as possible.
“Not only is PCT a valuable tool for helping to identify sepsis early in the course of the condition, it is now recognized as a valuable tool for identifying sepsis patients at the greatest risk of severe disease and mortality,” says Bozette. At the end of June, FDA cleared 4-day serial use of the Vidas PCT test to track patients’ PCT levels once they have been admitted to the hospital. The agency’s clearance was based on findings of the procalcitonin monitoring sepsis study (MOSES), which tracked the PCT levels of patients admitted to intensive care units with severe sepsis or septic shock. Patients with low initial PCT levels that decreased by 80% or more during the 96-hour timeframe of the study had a significantly lower risk of 28-day mortality than patients whose daily PCT measurements decreased by less than 80% over 96 hours.

Daniel J. Feinstein, MD, FACP, Moses H. Cone Memorial Hospital
A recent study among septic patients found that PCT kinetics over the first 72 critical-care hours provide prognostic information beyond that available from clinical risk scores.15 “We have been using PCT for five years,” says Daniel J. Feinstein, MD, FACP, an internist specializing in critical care medicine at Moses H. Cone Memorial Hospital, a 535-bed tertiary care facility located in Greensboro, NC. “We have been able to reduce our protocol for antibiotic use from 5 days to 4 days, resulting in decreased length of stay and mortality with substantial cost savings to our institution,” says Feinstein.

Mark Miller, MD, bioMérieux.
“Meningitis is another potential cause of sepsis, and it is critical that it be identified quickly,” says Mark Miller, MD, chief medical officer at bioMérieux. BioMérieux’s meningitis/encephalitis panel tests cerebrospinal fluid for the most common bacteria, viruses, and fungi responsible for community-acquired meningitis or encephalitis (see Figure 5). “The panel takes about an hour to run on BioFire’s FilmArray molecular testing platform, a fully automated system that combines highly multiplexed PCR and melt curve analysis,” says Miller.
CONCLUSION
The incidence of sepsis has been increasing, particularly in inpatient settings. It is critical that causes of sepsis be identified rapidly so that targeted therapy can be initiated in a timely manner. Recent advances in bacterial, fungal, and viral detection methods have become important tools in the fight against sepsis.
Craig C. Foreback, PhD, is a contributing writer and member of the CLP editorial advisory board. For further information, contact chief editor Steve Halasey via [email protected].
REFERENCES
- Sepsis [online]. Atlanta: Centers for Disease Control and Prevention, 2016. Available at: www.cdc.gov/sepsis. Accessed August 25, 2016.
- Torio CM, Andrews RM. National inpatient hospital costs: the most expensive conditions by payor, 2011. Healthcare Cost and Utilization Project, statistical brief 160. Rockville, Md: Agency for Healthcare Research and Quality, 2013. Available at: www.hcup-us.ahrq.gov/reports/statbriefs/sb160.jsp. Accessed August 25, 2016.
- American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference: definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Crit Care Med. 1992;20(6):864–874.
- Vincent JL, Opal SM, Marshall JC, Tracey KJ. Sepsis definitions: time for change. Lancet. 2013;381(9868):774–775; doi: 10.1016/S0140-6736(12)61815-7.
- Shankar-Hari M, Phillips GS, Levy ML, et al., for the Sepsis Definitions Task Force. Developing a new definition and assessing new clinical criteria for septic shock: for the third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. 2016;315(8):775–787; doi: 10.1001/jama.2016.0289.
- Gaieski DF, Mikkelsen ME, Band RA, et al. Impact of time to antibiotics on survival in patients with severe sepsis or septic shock in whom early goal-directed therapy was initiated in the emergency department. Crit Care Med. 2010;38(4):1045–1053; doi: 10.1097/ccm.0b013e318cc4824.
- Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. 2016;315(8):801–810; doi: 10.1001/jama.2016.0287.
- Chan P, Peake S, Bellomo R, Jones D. Improving the recognition of, and response to in-hospital sepsis. Curr Infect Dis Rep. 2016;18(7):20; doi: 10.1007/s11908-016-0528-7.
- Lueangarun S, Leelarasamee A. Impact of inappropriate empiric antimicrobial therapy on mortality of septic patients with bacteremia: a retrospective study. Interdiscip Perspect Infect Dis. 2012;2012:765205; doi: 10.1155/2012/765205.
- Kumar A, Roberts D, Wood KE, et al. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit Care Med. 2006;34(6):1589–1596.
- Dekmezian M, Beal SG, Damashek MJ, Benavides R, Dhiman N. The SUCCESS model for laboratory performance and execution of rapid molecular diagnostics in patients with sepsis. Proc (Bayl Univ Med Cent). 2015;28(2):144–150.
- Koncelik DL, Hernandez J. The impact of implementation of rapid QuickFISH testing for detection of coagulase-negative staphylococci at a community-based hospital. Am J Clin Pathol. 2016;145(1):69–74; doi: 10.1093/ajcp/aqv005.
- Montull B, Menendez R, Torres A, et al. Predictors of severe sepsis among patients hospitalized for community-acquired pneumonia. PLoS One. 2016;11(1):e0145929; doi: 10.1371/journal.pone.0145929.
- Mylonakis E, Clancy CJ, Ostrosky-Zeichner L, et al. T2 magnetic resonance assay for the rapid diagnosis of candidemia in whole blood: a clinical trial. Clin Infect Dis. 2015;60(6):892–899; doi: 10.1093/cid/ciu959.
- Schuetz P, Maurer P, Punjabi V, Desai A, Amin DN, Gluck E. Procalcitonin decrease over 72 hours in US critical care units predicts fatal outcome in sepsis patients. Crit Care. 2013;17(3):R115; doi: 10.1186/cc12787.




{kind=link}