
Emerging diseases exacerbate safe blood challenge
By Gary Tufel
For blood banks that are responsible for collecting, testing, and distributing blood and blood products to healthcare providers, protecting the safety of the blood supply is an ongoing challenge. Longstanding issues for blood banks include seasonal blood shortages, an ongoing dearth of trained personnel, the adoption of automated systems, and the need to control costs. But in recent years, those challenges to the safety of the nation’s blood supply have been joined by others, including a rising understanding of the risks involved in blood transfusions, threats related to known infectious diseases, and the emergence of new pathogens.
“In the past decade, the American Association of Blood Banks (AABB) and its members have addressed a number of blood safety issues,” says Steven H. Kleinman, MD, senior medical advisor to AABB and clinical professor of pathology and laboratory medicine at the University of British Columbia, Vancouver. “In addition to coordinating the implementation of tests for new or emerging infectious disease threats, we have also taken steps to address such issues as bacterial contamination of platelets and blood components, and other more-complex risks, such as transfusion-related acute lung injury.”

Aryeh Shander, MD, FCCM, FCCP, Englewood Hospital and Medical Center, Icahn School of Medicine.
“The original challenges still remain,” says Aryeh Shander, MD, FCCM, FCCP, chief of anesthesiology, critical care medicine, pain management, and hyperbaric medicine at Englewood Hospital and Medical Center, and executive medical director of the hospital’s institute for patient blood management and bloodless medicine and surgery. “Rising challenges include new pathogens entering the blood supply, and the need to develop ways to mitigate those risks. Inventory was another major challenge faced by blood banks, but with the use of transfusions dropping, that is now less of an issue than in the past.”1
BLOOD SHORTAGES
Summer has always been a tough time of the year for blood banks. High schools and colleges that often hold blood drives are out of session, and many regular donors go on vacation. Regardless of the season, however, healthcare providers’ need for blood and blood products remains strong, and patients continue to depend on the generosity of blood donors to meet that need. All blood types are needed.

Miriam A. Markowitz, MSc, AABB.
“Maintaining a safe and adequate blood supply is critical to the nation’s public health and a priority for the medical community,” says Miriam A. Markowitz, CEO of AABB. “Every 2 seconds, someone in the United States needs blood. It is indispensable and required in the treatment of millions of patients, including individuals with cancer and other life-threatening diseases, patients undergoing organ transplants, and trauma victims.”
This year, a couple of new factors have aggravated the expected seasonal shortage. The ongoing Zika outbreak in the Western hemisphere, and its gradual march toward gaining a toehold in the mainland United States, has raised significant questions about who should be permitted to donate blood and how blood donations should be tested for the Zika virus. Also complicating shortages this year are new donor rules requiring that male donors have a hemoglobin level of at least 13.0 g/dL—an increase over the previous requirement of 12.5 g/dL.
With such challenges on the horizon, authorities wasted little time before appealing for help in overcoming this summer’s shortages. In the middle of July, AABB issued a critical appeal for blood and platelet donors across the country. With the nation’s blood supply facing significantly low inventory levels, the blood community encouraged individuals throughout the United States to schedule an appointment to donate blood.2
STAFF SHORTAGES AND AUTOMATION
“One of the biggest challenges facing our customers in blood banks and transfusion service labs right now is the need to find skilled medical technologists,” says Heidi Casaletto, vice president of transfusion medicine at Ortho Clinical Diagnostics, Raritan, NJ. “Around the world, fewer and fewer medtechs are graduating from universities, and those who do graduate are often drawn to research roles rather than to hospital lab work.
“On a practical level,” Casaletto adds, “this means that, more than ever, our customers need automated solutions that can help labs type and screen patients and blood donors quickly and accurately, even in the face of staffing pressures.”

Eva Quinley, MS, MT(ASCP), SBB, Medic Regional Blood Center, LifeSource/ITxM.
“Some blood bankers have had to get over a dislike or fear of automation,” says Eva Quinley, MS, MT(ASCP), SBB, chief operating officer of Medic Regional Blood Center, Knoxville, Tenn, and executive director of LifeSource/ITxM, Chicago. “When I was first in a blood bank there was very little automation. Today, automation is a key element of most blood banks.”
“In order to type and screen blood for compatibility, we are seeing most hospital transfusion service labs around the world move their practices away from manual tube testing to the use of automated instrumentation,” agrees Casaletto. “This shift is being driven mostly by challenges in finding skilled labor, together with the continuous drive to improve patient outcomes by increasing safety (see Figure 1).

Figure 1. The Ortho Vision analyzer by Ortho Clinical Diagnostics automates the full range of immunohematology testing. It permits continuous access to load stat and routine samples, reagents, and consumables.
“A major challenge in adopting automation has been in training people to adopt a new way of working (see the companion article “Improving How Blood Banks and Clinical Labs Interact”). Manual and semiautomated approaches often push the lab to create workarounds in order to be efficient and effective,” adds Casaletto. “Today’s automation solutions should be carefully and thoughtfully implemented so that they mirror the way the lab actually operates. That takes time and energy during implementation, but it can create significant efficiency benefits down the road.”
The increased use of automated systems in blood banks has correspondingly raised the need to validate those automated processes, to ensure that test results are accurate and reliable, observes Quinley.
One of the most significant challenges raised by the increased use of automation over the past decade, says Kleinman, is how to interface automated blood banking systems with a facility’s laboratory information system (LIS). “This challenge is mainly due to the existence of multiple vendors that supply blood bank and clinical laboratory software, as well as the regulatory requirements that apply to blood bank information systems,” he adds.
Like clinical laboratories, blood collection organizations and blood banks rely heavily on automation, says Kleinman. “New technology allows new infectious disease tests to be rapidly implemented in bulk. This approach has also been applied to blood grouping. It allows for the use of complex informatics-based labeling schemes.”3–5

Heidi Casaletto, Ortho Clinical Diagnostics.
Automation technologies have made it possible to screen and type blood in an accurate, timely manner in order to ensure that a proper, safe match can be made from donor to recipient, says Casaletto. “The next step is to harness technology to do two things. First, to perform much more detailed screening—to go beyond typing and screening, to ensure that the patient has as perfect a match as possible, every time. And second, to automate and digitize the process, to ensure that fast, accurate, detailed screening can occur even in the face of challenges such as staffing shortages or consolidation.”
SAFEGUARDING THE BLOOD SUPPLY IN STORAGE
Safeguarding the blood supply is made all the more challenging by the fact that risks can come from several different directions. To optimize the use of plasma, platelets, and red blood cells, for instance, it is critical to have accurate and reliable temperature control as well as appropriate containers. In the case of platelets, recent product advances have led to an increase in the number of days that the cells can be stored before use.

Colleen Holtkamp, MBA, Helmer Scientific.
“Platelets are small cells that circulate within the blood. Their principal function is to prevent bleeding,” explains Colleen Holtkamp, market manager at Helmer Scientific, Noblesville, Ind. “Platelets bind to the site of a damaged vessel, causing a blood clot in order to stop bleeding.”
Donated platelets are used to treat thrombocytopenia, a condition in which there is a shortage of platelets, and to treat platelet-function abnormalities. They are essential for patients fighting cancer, chronic diseases, and traumatic injuries.
Platelet products must be stored at room temperature with gentle agitation. “In the past this requirement has limited the shelf-life of platelet products to 5 days because of the risk of bacterial growth in a room-temperature environment,” says Holtkamp. “However, regulatory developments have made it possible to extend the shelf-life of certain platelet products to 7 days. Recent changes include FDA clearance of two 7-day storage containers and a secondary safety test.”

Figure 2. The Helmer Blood Bank Refrigerator model iB125 has a 504 blood bag capacity, and features a full-color touchscreen monitor with downloading capability.
The secondary test is a critical safety measure performed at the hospital within a 24-hour window prior to a platelet transfusion. It prevents the transfusion of contaminated units that have not been detected by the culture-based method used soon after collection.
A recent FDA guidance document provides recommendations on how to control the risk of bacterial contamination for platelets stored at room temperature and includes information on extending the expiration date to 7 days, Holtkamp says.6,7 This practice is beneficial to transfusion services because the longer shelf-life makes it easier to manage expiration dates and reduce waste of a precious resource.
“These clearances and regulatory changes have paved the way for the use of 7-day platelets, enhancing patient safety and saving the US healthcare system millions of dollars annually,” says Holtkamp.
“Another important element of risk reduction for blood banks is the use of high-quality temperature-controlled storage equipment and processing devices,” says Holtkamp (see Figure 2). “Systems such as these advance patient safety, compliance, and efficiency.”

Figure 3. The BloodTrack HaemoBank 80, codeveloped by Helmer Scientific and Haemonetics, offers just-in-time blood allocation solutions that act as 24/7 virtual, automated blood banks, helping to reduce blood bank workload, safely improve access, and reduce waste.
Vendors have also made advances in remote blood storage, says Holtkamp. Helmer’s BloodTrack HaemoBank, codeveloped by Haemonetics, Braintree, Mass, is a just-in-time remote blood allocation solution that provides clinicians with access to individual blood products where and when they are needed (see Figure 3).
“The BloodTrack HaemoBank provides bin-level cold storage, and is designed for departments or remote sites administering transfusions,” Holtkamp explains. “The solution enables those sites to store and remotely allocate uncrossmatched ABO-Rh blood groups, along with crossmatched and labeled units, and emergency products, at the point-of-use.”
THE RISKS OF TRANSFUSION
Transfusions are risky because the body’s immune system reacts to them as a foreign object analogous to an organ transplant, says Eleanor Herriman, MD, MBA, chief medical informatics officer at Viewics Inc, Sunnyvale, Calif. As a result of such immune system responses, the rate of infections, heart problems, lung problems, and death increases.

Eleanor Herriman, MD, MBA, Viewics Inc.
“This has always been an issue, but it has only been in the past decade or so that scientists have discovered the problem and raised awareness about it,” says Herriman. “The strategy for mitigating this problem involves restricting the use of transfusions to those patients who absolutely need them, as well as restricting the amount of blood transfused. This approach is generally termed blood program management (see the companion article “Analytics Capabilities for Blood Management Programs”).”
Excessive transfusion utilization is a major, widespread problem associated with high rates of morbidity, mortality, and avoidable spending. But some institutions have now put in place evidence-based restrictive guidelines and blood programs that can change clinician practice patterns and generate significant clinical value.
According to Shander, blood transfusion is far riskier than people believe, and is responsible for billions in wasted healthcare dollars every year. But in the United States, the blood transfusion problem has been recognized for quite a long time. A 1999 New England Journal of Medicine article was among the earliest studies to question the efficacy of blood transfusion, and the peer-reviewed literature now includes dozens of clinical trials indicating that when it comes to saving lives and improving outcomes—as well as preventing wasted dollars—less transfusion is more.8
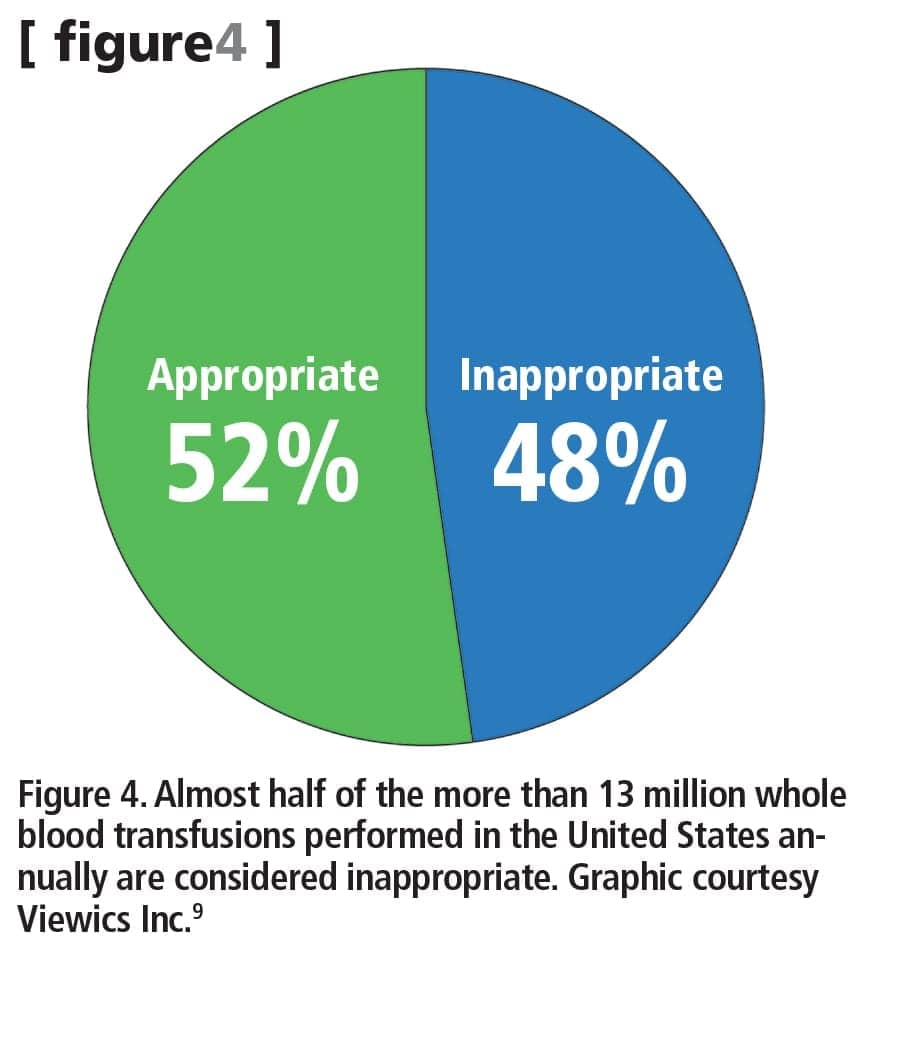
Figure 4. Almost half of the more than 13 million whole blood transfusions performed in the United States annually are considered inappropriate. Graphic courtesy Viewics Inc.9 Click to expand.
Recent data show that almost half of transfusions performed in the United States should be deemed inappropriate (see Figure 4).9 In another study of the morbidity and mortality impact of transfusion practices, the risk of mortality was found to be about 26% higher when a hospital followed a liberal policy with regard to transfusions. Total mortality—including death after hospitalization—was found to be 20% higher (see Figure 5).10
Moreover, the study found that liberal transfusion practices resulted in a 36% higher risk of rebleeding, a 56% higher incidence of acute coronary syndrome, a 52% higher rate of pulmonary edema, and a 14% higher rate of bacterial infections.
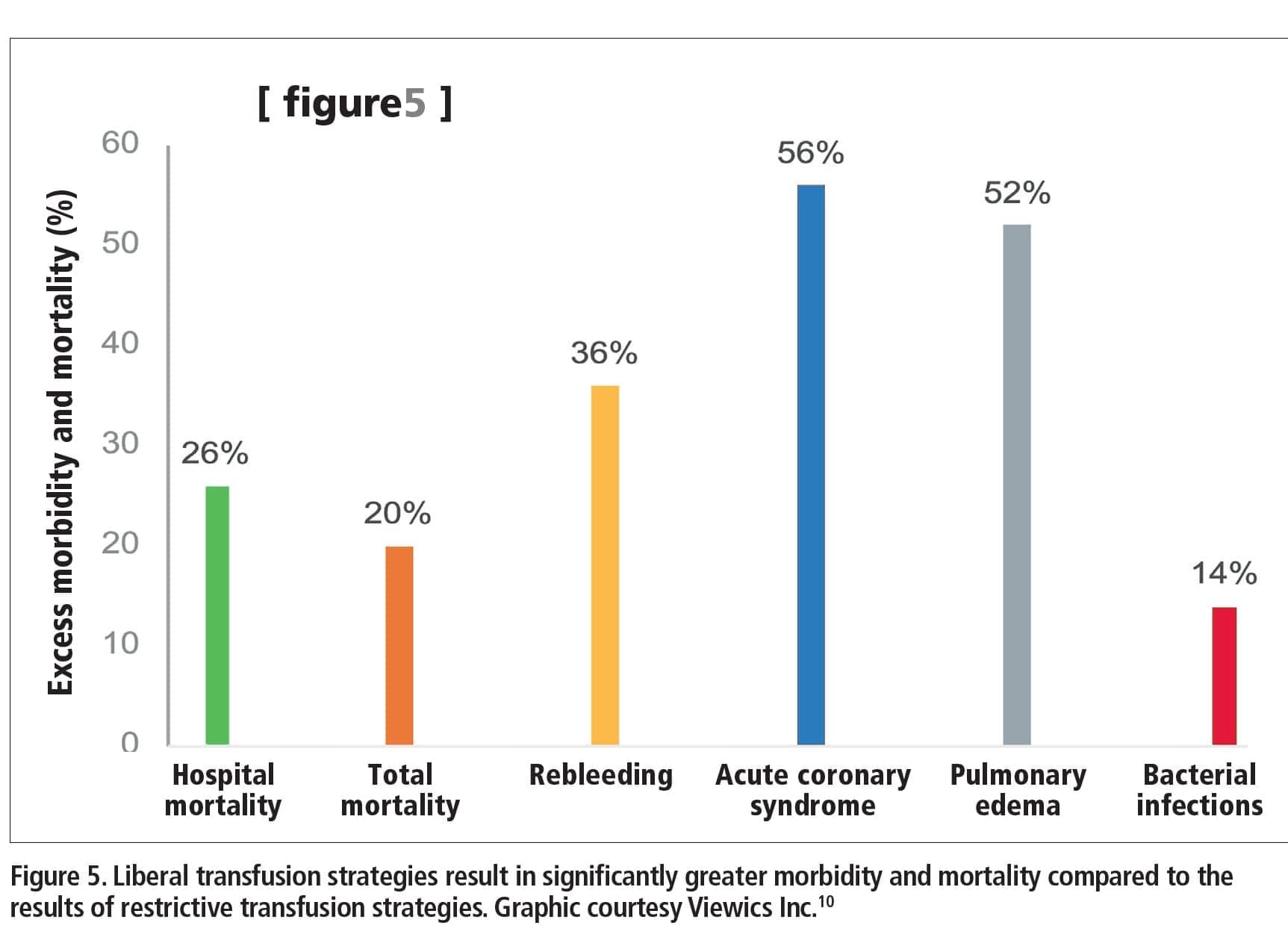
Figure 5. Liberal transfusion strategies result in significantly greater morbidity and mortality compared to the results of restrictive transfusion strategies. Graphic courtesy Viewics Inc.10 Click to expand.
Despite such a growing acknowledgment of the risks inherent in the use of transfusions, adopting new guidelines to restrict the practice continues to be a struggle for healthcare providers.11 Today’s practicing physicians were trained in accord with older guidelines that recommended a more liberal transfusion trigger. And a number of studies have suggested that it takes about 17 years for physicians to adopt new practice guidelines.12 Consequently, there is wide variation in ordering transfusions, which is not uncommon in medicine, says Herriman.
In the past, a hemoglobin level of 8–12 g/dL was considered an acceptable trigger for performing a transfusion, depending on the setting. Also, past guidelines recommended that physicians start by transfusing two units of blood. Newer clinical guidelines recommend that physicians adopt a more-restrictive level of 7–8 g/dL as the trigger for performing a transfusion on stable, hospitalized patients, and that they start with only one unit of blood.13
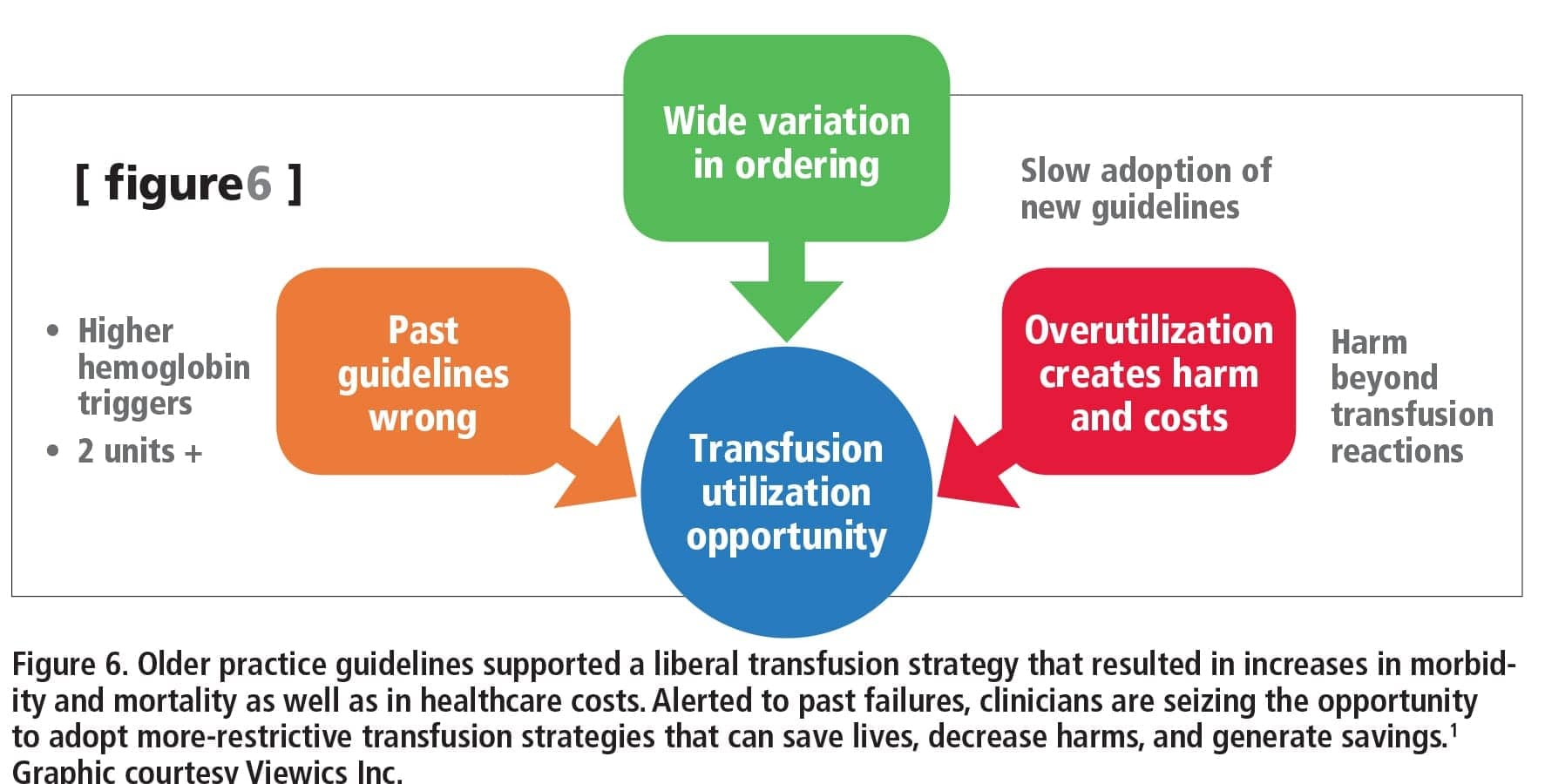
Figure 6. Older practice guidelines supported a liberal transfusion strategy that resulted in increases in morbidity and mortality as well as in healthcare costs. Alerted to past failures, clinicians are seizing the opportunity to adopt more-restrictive transfusion strategies that can save lives, decrease harms, and generate savings. Graphic courtesy Viewics Inc.1 Click to expand.
Some physicians have adopted the newer guidelines, while others have not. But the magnitude of potential harms associated with older transfusion guidelines go way beyond the classic transfusion reaction, raising physician awareness of the resulting increases in morbidity and mortality as well as healthcare costs (see Figure 6). “Put all of this together, and what you have is a tremendous opportunity to drive adoption of these new programs and guidelines, and save lives, decrease harms, and generate savings,” says Herriman.
A study of transfusions related to hip and knee replacements in 345 hospitals found wide variation—from 5% to 100%—in the percentage of patients receiving transfusions. The researchers calculated that, on average, if a hospital were to impose a restrictive transfusion policy on just the hip and knee replacements its providers perform, the institution could save $1 million a year, including not only the cost of the blood, but also the reduced costs resulting from decreases in patient mortality, length of stay, and other adverse events.14
At the same time, more people are living with chronic diseases and undergoing multiple surgeries. “This means more patients are being exposed to multiple blood transfusions. As a result, we are seeing alloimmunization as an increasing risk, creating difficulties in matching blood between donor and recipient, and a higher risk of life-threatening and lifelong consequences,” says Casaletto. “We need to counter this risk with better matching in the long term to minimize complications down the line,” she says.
INFECTIOUS DISEASES AND THE BLOOD SUPPLY
Emerging infectious diseases represent enormous challenges to the safety of the blood supply. This year, probably no single pathogen is more emblematic of those challenges than the Zika virus. After more than a year filled with surprises related to the spread of the Zika virus, especially in the Western hemisphere, in August FDA’s Center for Biologics Evaluation and Research issued a revised guidance document on reducing the risk of Zika virus transmission through donated blood and blood components.15 Recommendations included testing all blood collected in the United States and its territories for the Zika virus.
Marked “for immediate implementation,” the new guidance takes into account fresh findings about how the virus is spread, and supersedes agency recommendations from earlier in the year. The agency concludes that the risk of Zika virus transmission by blood transfusion is considered likely, and cites a number of studies to support key evidence.16
Ease of international travel has resulted in additional exposure to infectious agents, which in turn results in deferral of blood donorship and a shrinking donor supply. “Dealing with emerging infectious diseases has presented a new set of challenges,” says Quinley. “Protecting the blood supply from such pathogens has required blood banks to ask additional questions about prospective blood donors and their possible exposure to emerging infectious diseases, and to implement additional testing for the new pathogens—if indeed appropriate tests are available. Again, additional donor deferrals and economic pressures have resulted.”
Special considerations will be necessary to continue protecting donated blood and organs from emerging infectious diseases, including antibiotic-resistant organisms. According to Quinley, such considerations should include whether a test is available, whether testing should be universal or selective, when to implement a test, how to handle positive test results (including donor counseling), the financial impact on the blood bank, and whether the blood bank has the resources to perform testing if implementation is not mandatory.

Steven H. Kleinman, MD, University of British Columbia.
“As the current concern about Zika virus illustrates, there will continue to be safety concerns related to emerging infectious agents,” adds Kleinman. “It is logistically difficult to continually develop new donor screening tests, and it is expensive for the manufacturers of such tests to obtain FDA approval.
“In the blood donation setting, an evolving approach is the use of broad-based pathogen reduction technology (PRT), which can inactivate a wide variety of blood-borne pathogens,” says Kleinman. “This technology is licensed in the US for application to platelets and plasma, but is still under evaluation for red blood cells. As with testing, however, implementation of this newer approach is expensive. Furthermore, this approach is not applicable to organ transplantation.”
Despite its current limitations, says Englewood hospital’s Shander, PRT will never go away. Currently available methods can be improved so that they more effectively protect against a greater number of pathogens, but their effectiveness will never be 100%. Ongoing research is promising, says Shander, but some have expressed concern that some pathogen reduction processes might bring about unforeseen and unintended consequences.
“The most significant challenge is to find the healthcare resources to pay for such additional safety steps,” says Kleinman. “The system that provides monetary reimbursement to hospitals has not taken into account the cost of these safety interventions, nor have hospitals been entirely willing to spend their own funds to decrease risks that are already quite low.”
“A major challenge here is to take a systemic approach, and look at the efficiency with which the blood supply is tested,” says Casaletto. “We are seeing consolidation among the blood donor centers, so it’s important that they adopt flexible, scalable, integrated systems. Automation, and eventually digitization, will help minimize errors and allow blood banks to keep pace with change.”
THE OUTLOOK FOR MEETING BLOOD BANK CHALLENGES
“As you can see with current state of Zika virus research and testing, the challenges for the blood supply are ongoing, and I don’t see them as ever resolving or being resolved,” says Shander. “Protecting the safety of the blood supply is a work in progress that requires constant vigilance and surveillance.
“All this raises the question of who really needs to be transfused, and whether there are other safe and effective treatments that answer the needs of patients, without defaulting to blood transfusions,” Shander adds. “The answer is yes—but that is where we are lagging.”
One of the major ways that blood banks have overcome the challenges facing them is to learn from one another, so that they are not continuously reinventing the wheel. Another way has been to ask vendors to develop the tools and training needed to facilitate the implementation of new technologies. “This has made implementation of new technology much easier,” says Quinley.
New blood banking technologies and instrumentation are designed to improve the safety and reliability of test results, and they have certainly helped transfusion centers and hospitals cope with staffing pressures, says Casaletto. “Automated analyzers can minimize the number of complex steps required to perform a test—especially when compared to manual tube testing—and can accurately run and interpret results.
“Every lab that implements an automated system will experience a slight difference in the associated savings and efficiencies, depending on the volume and type of tests they run,” says Casaletto. “But the literature published in numerous industry white papers and presented at many conferences demonstrates that many successes have been achieved and documented.”
Gary Tufel is a contributing writer for CLP. For further information, contact CLP chief editor Steve Halasey via [email protected].
REFERENCES
- Herriman E. The United States’ risky blood transfusion problem [online]. Sunnyvale, Calif: Viewics Inc, 2016. Available at: https://viewics.com/blog/the-united-states-risky-blood-transfusion-problem/?utm_source=email&utm_medium=blog+digest&utm_campaign=blog+digest+may+2016. Accessed September 14, 2016.
- Significant shortages impact US blood supply [press release]. Washington, DC: American National Red Cross, 2016. Available at:
www.redcross.org/news/press-release/significant-shortages-impact-us-blood-supply
Accessed September 10, 2016.
- What is ISBT 128? [online]. San Bernardino, Calif: International Council for Commonality in Blood Banking Automation Inc. Available at: www.iccbba.org/home/isbt-128-basics/what-is-isbt-128. Accessed September 20, 2106.
- International Society of Blood Transfusion. ISBT 128 standard: technical specification, ver. 5.5.0. San Bernardino, Calif: International Council for Commonality in Blood Banking Automation Inc, 2016. Available at: www.iccbba.org/subject-area/tissues/technical-specification. Accessed September 21, 2016.
- United States industry consensus standard for the uniform labeling of blood and blood components using ISBT 128, ver. 3.0.0. San Bernardino, Calif: International Council for Commonality in Blood Banking Automation Inc, 2013. Available at: www.fda.gov/downloads/biologicsbloodvaccines/guidancecomplianceregulatoryinformation/guidances/blood/ucm079159.pdf. Accessed September 21, 2016.
- Holtkamp C. The FDA has opened the door for 7-day platelet storage [online]. Noblesville, Ind: Helmer Scientific, 2016. Available at: http://blog.helmerinc.com/seven-day-platelet-storage. Accessed September 14, 2016.
- Draft guidance for industry: bacterial risk control strategies for blood collection establishments and transfusion services to enhance the safety and availability of platelets for transfusion. Silver Spring, Md: Center for Biologics Evaluation and Research, FDA, 2016. Available at www.fda.gov/downloads/biologicsbloodvaccines/guidancecomplianceregulatoryinformation/guidances/blood/ucm425952.pdf. Accessed September 16, 2016.
- Goodnough LT, Brecher ME, Kanter MH, AuBuchon JP. Transfusion medicine, part 1: blood transfusion. N Engl J Med. 1999;340:438–447; doi: 10.1056/nejm199902113400606.
- Hannon T, Sikka R. Commentary: saving blood, dollars, and lives [online]. WSJ. January 15, 2015. Available at: www.wsj.com/articles/tim-hannon-and-rishi-sikka-saving-blood-dollars-and-lives-1421366642. Accessed September 20, 2016.
- Salpeter SR, Buckley JS, Chatterjee S. Impact of more restrictive blood transfusion strategies on clinical outcomes: a meta-analysis and systematic review. Am J Med. 2014;127(2):124–131; doi: 10.1016/j.amjmed.2013.09.017.
- Blood safety basics [online]. Atlanta: Centers for Disease Control and Prevention, 2011. Available at: www.cdc.gov/bloodsafety/basics.html. Accessed September 14, 2016.
- Morris ZS, Wooding S, Grant J. The answer is 17 years, what is the question: understanding time lags in translational research. J R Soc Med. 2011;104(12):510–520; doi: 10.1258/jrsm.2011.110180.
- Carson JL, Grossman BJ, Kleinman S, et al. Red blood cell transfusion: a clinical practice guideline from the AABB. Ann Intern Med. 2012;157(1):49–58; doi: 10.7326/0003-4819-157-1-201206190-00429.
- Koppenheffer M. There will (not) be blood: big opportunity to cut blood use in knee and hip cases [online]. Washington, DC: The Advisory Board Co, 2015. Available at www.advisory.com/research/physician-executive-council/prescription-for-change/2015/06/there-will-not-be-blood. Accessed September 14, 2016.
- Guidance for industry: revised recommendations for reducing the risk of Zika virus transmission by blood and blood components. Silver Spring, Md: Center for Biologics Evaluation and Research, FDA, 2016. Available at: www.fda.gov/downloads/biologicsbloodvaccines/guidancecomplianceregulatoryinformation/guidances/blood/ucm518213.pdf. Accessed August 31, 2016.
- Halasey S. From the editor: new guidance on Zika testing. Clinical Lab Products. 2016;46(9):6. Available at: www.clpmag.com/2016/08/editor-new-guidance-zika-testing. Accessed September 10, 2016.



{kind=link}