
Blood-based genomic tests are improving treatment decision and start times
By Krish Bhadra, MD, Hestia Mellert, PhD, and Gary Pestano, PhD
Lung cancer prognoses are typically measured in months. About 75% of lung cancer patients are diagnosed at an advanced stage, when surgical removal of a tumor is rarely sufficient, if indeed possible, due to metastasis.1,2 For treating advanced stage non-small cell lung cancer (NSCLC)—the most common form of lung cancer—the emerging standard of care is to test for biomarkers and use drugs that specifically target them. Generalized therapies such as chemotherapy or radiation therapy are less effective, because not all NSCLCs share the same types of mutations driving cancer growth.3,4 For optimal results, treatment must be tailored to each patient, and the sooner that targeted treatment begins, the greater the chance of survival.5
However, delays in targeted treatment remain a challenge. Because of long wait times for biopsy results—typically over 3 weeks—four out of five patients do not have tumor-specific data at their first oncology consultation, normally scheduled within the first 2 weeks after diagnosis.6

Krish Bhadra, MD, CHI Memorial Medical Group.
To expedite biomarker test results and improve NSCLC treatment, molecular testing company Biodesix Inc, Boulder, Colo, has collaborated with five cancer centers across the United States to test the clinical utility of its liquid biopsy test, GeneStrat. Each member of this multidisciplinary thoracic oncology working group has adopted the same blood-based testing strategy, and will gather and publish data within their respective communities on the effectiveness of the GeneStrat test in conjunction with selected therapies. The working group includes CHI Memorial Hospital, Chatanooga, Tenn; Gundersen Lutheran Medical Center, La Crosse, Wisc; Leo Jenkins Cancer Center, Greenville, NC; Pinehurst Medical Clinic, Pinehurst, NC; and 21st Century Oncology (a national cancer care services provider).
The tests adopted by the working group members incorporate genomic and proteomic analyses of blood from NSCLC patients to identify genetic mutations that can determine targeted treatment plans. Since 2015, data from 179 GeneStrat tests ordered for lung cancer patients from the five collaborating centers have been analyzed by pulmonologist Mark R. Bowling, MD, FCCP, assistant professor and chief of pulmonary, critical care, and sleep medicine, and oncologist Paul R. Walker, MD, FACP, associate professor and chief of hematology/oncology, both members of the working group from East Carolina University. Among the physicians ordering the tests, 95% received results within 72 hours of ordering; average time to results was 33 hours.5 Mutation results that had an impact on patient management were found in 20% of test results.6

Hestia Mellert, PhD, Biodesix Inc.
The quick turnaround for such test results led to shorter median times to treatment decision (0 vs. 22 days) and earlier treatment start times (16 vs. 29 days) when compared to the absence of this information. With biomarker results in hand weeks earlier than normal, physicians can work more efficiently within the tumor board to coordinate treatment decisionmaking at the first oncology appointment, significantly improving patient care.7
Liquid and Tissue: Partners for Complete Analysis
As promising as liquid biopsy is, the gold standard for cancer diagnosis remains tissue biopsy, because histology is such a vital part of diagnosing and subtyping cancers. Additionally, liquid biopsy technologies often struggle to detect mutations in cancers that do not shed much DNA, such as very small, early-stage tumors. Thus, liquid biopsy is unlikely to replace tissue biopsy until detection technologies advance significantly, along with our understanding of histology-specific molecular alterations.8
Nevertheless, liquid biopsy can be particularly effective when used in conjunction with a tissue biopsy as a powerful, complementary technique. A blood sample taken the same day as a tissue biopsy adds rapid genotyping to histological data, forming a comprehensive picture of the cancer at the start of treatment.
Early Results Facilitate Medical Collaboration
Availability of biomarker data early in the treatment process enables tumor boards to review cases more efficiently and to better understand treatment options. The five cancer centers that banded together with Biodesix in May 2016 to form the multidisciplinary thoracic oncology working group are experiencing this at first hand.
Working group pulmonologist Michael Pritchett, DO, of Moore Regional Hospital and Pinehurst Medical Clinic in North Carolina, reports that his practice has more sophisticated conversations because they are empowered with the ability to help fast-track patients. The interventional pulmonologist, the pathologist, and the oncologist, he says, can now speak the same language, and this improves communication with the patient as well.
Timely Care is Patient-Centric Care
Pritchett, who also serves as director of the chest center at Pinehurst Hospital, further reports that his practice is seeing a significant decrease in its rebiopsy rate, as well as in patient anxiety and wait time for test results.
Such improvements are crucial to patient-centric care, because for patients the process of getting a biopsy and waiting for results is riddled with significant anxiety and fear. Cancer does not take a day off, and most patients fear their cancer spreading with each passing day. Though progression of a tumor is seldom as fast as that, physicians nonetheless perform an important service when they seek to alleviate their patients’ stress by guarding against unexpected tumor aggression and treating the disease as efficiently as possible.
At the Leo Jenkins Cancer Center, early testing has resulted in patients starting treatment within 7 days of initial diagnostic biopsy or blood draw.5 Studies are ongoing to detail the effects of early intervention on overall survival for NSCLC patients. But it is clear that blood-based genomic testing earlier in the continuum of care can help patients receive appropriate treatment sooner (For more information, see “Liquid Biopsy at a Glance“).
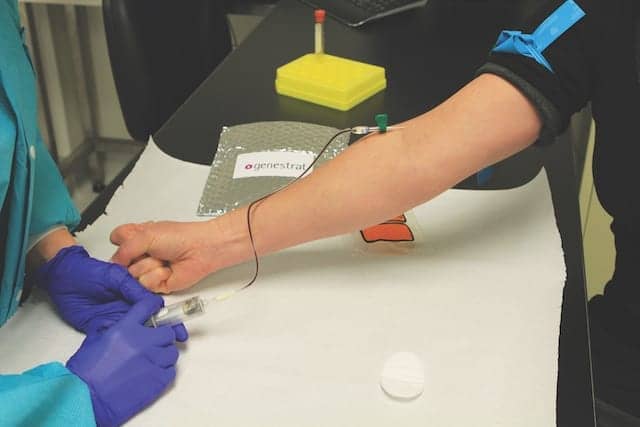
Figure 1. Phlebotomist collecting blood from a patient using the GeneStrat testing kit.
The painful procedure of a tissue biopsy is another source of emotional stress for patients, and in some cases it causes physical danger as well. The risk of lung collapse with transthoracic needle aspiration is significant, and rises with complicating conditions such as emphysema. Additionally, needle aspiration may require repeat procedures, as the sample is taken from only one location in the body. Though bronchoscopy mitigates those risks, it is a highly invasive procedure, and carries the same emotional weight to the patient.
Liquid biopsies such as the GeneStrat test, on the other hand, capture information from a minimally invasive blood draw, incurring less risk and inflicting less emotional trauma on the patient than tissue biopsy (see Figure 1).
Digital PCR Technology Overcomes Limitations
Compared to the abundant background of wild-type DNA from non-tumor sources, the proportion of cell-free circulating tumor DNA (ctDNA) in the blood is often very small. Such ctDNA is also typically highly fragmented, which further reduces the concentration of detectable intact target sequences. With such a small amount of starting material, false negatives present a potential source of error that could be as damaging to diagnosis as no information at all. Furthermore, the traces of sample recovered do not necessarily represent the entire tumor.

Figure 2. Biodesix technician processing test samples on Bio-Rad’s Droplet Digital PCR system.
Biotechnology firms are pushing back against these limitations. Bio-Rad Laboratories, Hercules, Calif, for example, has developed a Droplet Digital PCR technology (ddPCR) to achieve highly sensitive and absolute quantification of nucleic acids. In this workflow, nucleic acid samples from blood or any other source are partitioned into thousands of droplets using a water-oil emulsion system. Each droplet acts as a tiny, individual test chamber for nucleic acid amplification during polymerase chain reaction (PCR). By design, relatively few of the droplets include a target sequence. Amplification occurs in all droplets simultaneously, and a binary count of droplets (through fluorescence detection) that contain target sequences adjusted for Poisson distribution yields an absolute quantity of mutations.
Partitioning enables highly sensitive, rapid, and reproducible screening of target nucleic acid molecules present in low levels.9–11 Such ddPCR systems do not require large numbers of replicates, and run amplification reactions to endpoint, resisting the effects of inhibitors.12 Applied to liquid biopsy, these qualities bring marked improvements over methods based on quantitative real-time PCR (qPCR), which measure nucleic acids in unpartitioned samples, and rely on amplification reference curves for absolute quantification.
The ddPCR technology has been adopted by basic research labs and in clinical trials for liquid biopsy processing, particularly in the areas of breast cancer, melanoma, and NSCLC (see Figure 2).13–17 A recent study involving 180 advanced stage NSCLC patients found plasma ddPCR assays detected EGFR and KRAS mutations with the high specificity needed to decide therapy and avoid repeat biopsies. Median test turnaround time for plasma ddPCR was 3 days, compared to 12–27 days for tissue genotyping assays.18
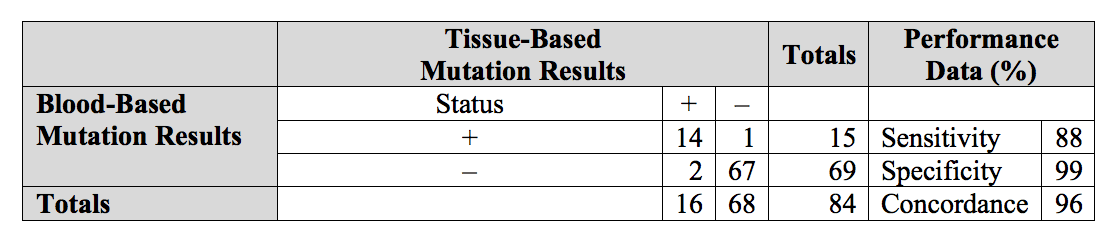
Table 1. Data comparing the GeneStrat test’s concordance with tissue-based testing. Click to expand.
Another clinical study conducted by the Gundersen Health System, La Crosse, Wisc, showed that the GeneStrat test, which uses ddPCR as the analysis platform, was highly concordant with tissue-based mutation results.16 When compared to tissue, GeneStrat had a sensitivity of 88%, specificity of 99%, and overall concordance of 96% (see Table 1).
Advances in next-generation sequencing (NGS) are similarly fast-tracking new innovation. Illumina spin-off Grail is reportedly pursuing an NGS-based test to detect asymptomatic tumors for multiple cancers. NGS forms the foundation of several other liquid biopsy tests that assess large genomic regions for detection of dozens of mutations, and this type of analysis allows for a far more comprehensive understanding of a cancer’s genetic makeup.
Critics, however, question the clinical utility of such large panels in cases where only a small number of those mutations are clinically actionable. By comparison, ddPCR-based liquid biopsies are often used to evaluate a targeted set of known, clinically actionable mutations with greater sensitivity.19 Claiming something of a middle ground, some groups, including one at the Dana-Farber Cancer Institute, have combined ddPCR and NGS techniques in their testing strategies in search of an optimal approach.20 The clinical utility of whole-genome profiling by NGS, paired with the focused, quantitative, and fast measurements by ddPCR, present a powerful amalgam for cancer care.
Negative results from either platform call for more information. Proteomic testing can elucidate a patient’s response to a growing tumor and the chronic activation of complex proteomic pathways linked to aggressive cancer. Biodesix’s VeriStrat test, which is a part of the company’s lung reflex testing strategy that includes the GeneStrat test, is used as a predictive and prognostic tool to assess proteomic information from patients with advanced NSCLC.
A Liquid Biopsy Testing Strategy in Action
A liquid biopsy test is less a magic bullet and more a critical piece of a modern treatment strategy. Biodesix’s lung reflex testing strategy integrates real-time measurement of genomic and proteomic biomarkers to inform tumor mutation status and the effects of the patients’ immune response to their tumors.
The GeneStrat test identifies clinically actionable driver mutations using Bio-Rad’s ddPCR platform, including EGFR sensitizing mutations (L858R and del19 E746-A750), EGFR resistance mutations (T790M), KRAS and BRAF mutations, and EML4-ALK, ROS1, and RET fusions. The term ‘driver’ comes from the fact that these over-expressed genes essentially drive the progression of cancer. Driver mutations are valuable finds because they tend to have targeted drugs; for example, several FDA-approved drugs are available to specifically treat an EGFR mutation. In a study carried out by the Gundersen Medical Center, 17.8% (n = 5) of patients who had submitted blood for GeneStrat testing had a treatable driver mutation.16
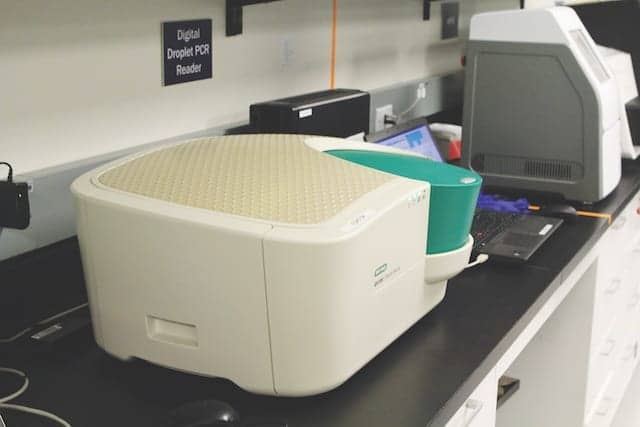
Figure 3. Bio-Rad QX200 Droplet Digital PCR system used for sample processing.
This precision medicine approach ensures that patients receive treatment personalized to the genetic profile of their particular cancer. A patient’s chance of survival can improve from months to several years—a promising difference to a Stage 4 patient who would normally have no hope whatsoever. What’s more, Biodesix is developing additional tests for more comprehensive coverage of DNA and RNA variants to mirror advances in drug discovery.
The blood-based testing process initiates with the use of a specimen collection kit provided by Biodesix. Day One of testing involves drawing whole blood into the provided specialized blood collection tubes and shipping the samples at ambient temperature to the Biodesix CLIA-certified laboratory for processing. During Day 2, the samples are logged into a secure laboratory information management system (LIMS) and passed through parallel workflows to isolate circulating DNA and RNA. The RNA is converted to cDNA using reverse transcription. Overnight, samples are processed using the Bio-Rad QX200 Droplet Digital PCR system (see Figure 3). Finally, on Day Three, the resulting data are analyzed for each variant in the GeneStrat test and reported to the ordering doctor. The whole process takes 3 days.21
Beyond Initial Diagnosis
When tissue biopsies do not furnish enough sample for every test that is needed, blood draws can offer a safer and easier alternative to rebiopsy. By avoiding unnecessary tissue biopsies, hospitals and clinics can reduce costs and minimize invasive tests. Likewise, when invasive traditional biopsies are deemed too risky for a patient in critical or fragile condition, a liquid biopsy provides a viable alternative. For these reasons, liquid biopsies make a great serial testing strategy for monitoring disease progression and therapeutic effects.

Gary Pestano, PhD, Biodesix Inc.
The future of liquid biopsy testing holds promise in guiding new forms of therapy. One Biodesix development in the works is the addition of programmed death ligand-1 (PD-L1) to the GeneStrat test’s panel of targets.22 As an immune checkpoint protein, PD-L1 has gathered a tremendous amount of interest for its therapeutic potential. The ability to detect the PD-L1 status of a patient from his or her blood will open doors for immunotherapy solutions to lung cancer management.
In any application, the speed of liquid biopsy testing will be what matters. Fast access to molecular information transforms clinical practices into agile, modern teams that can accelerate treatment when time is precious, which is why hospitals and clinics are increasingly offering the option of liquid biopsy testing to patients. Though careful planning is warranted before implementing this type of testing in a practice, the momentum of adoption is clear. Clinical trials are showing reliable data and positive outcomes, and the data are growing.
Krish Bhadra, MD, is an interventional pulmonologist at CHI Memorial Medical Group; Hestia Mellert, PhD, is senior scientist and project manager for product development at Biodesix Inc; and Gary Pestano, PhD, is vice president for product development and operations at Biodesix Inc. For further information contact CLP chief editor Steve Halasey via [email protected].
References
- Hurria A, Kris MG. Management of lung cancer in older adults.CA Cancer J Clin. 2003;53(6):325–341.
- Lung Cancer Screening Programs. Atlanta: National Center for Chronic Disease Prevention and Health Promotion, Centers for Disease Control and Prevention, [n.d.]. Available at: www.cdc.gov/cancer/ncccp/pdf/lungcancerscreeningprograms.pdf. Accessed April 30, 2017.
- Treatment Choices for Non-Small Cell Lung Cancer, by Stage [online]. Atlanta: American Cancer Society, 2016. Available at: www.cancer.org/cancer/non-small-cell-lung-cancer/treating/by-stage.html. Accessed April 30, 2017.
- Kegel M. Blood test at lung cancer diagnosis shortens time to treatment decisions.Lung Cancer News Today. November 3, 2016. Available at: https://lungcancernewstoday.com/2016/11/03/blood-test-at-lung-cancer-diagnosis-shortens-time-to-treatment-decision.
- Bowling M, Mattingley J, Bhadra K, Pritchett M, Skibo S, Walker PR. PSO1.16: Shortening time from diagnosis to treatment in NSCLC: are blood-based biopsies the answer?J Thorac Oncol. 2016;11(11_S):S278–S279; doi: 10.1016/j.jtho.2016.09.051.
- Lim C, Tsao MS, Le LW, et al. Biomarker testing and time to treatment decision in patients with advanced nonsmall-cell lung cancer.Ann Oncol. 2015;26(7):1415–21; doi: 10.1093/annonc/mdv208.
- Schwaederle M, Parker BA, Schwab RB, et al. Molecular tumor board: the University of California, San Diego, Moores Cancer Center experience. Oncologist. 2014;19(6):631–636; doi: 10.1634/theoncologist.2013-0405.
- Mino-Kenudson M. Cons: can liquid biopsy replace tissue biopsy?—the US experience.Transl Lung Cancer Res. 2016;5(4):424–427; doi: 10.21037/tlcr.2016.08.01.
- Watanabe M, Kawaguchi T, Isa S, et al. Ultra-sensitive detection of the pretreatment EGFR T790M mutation in non–small cell lung cancer patients with an EGFR-activating mutation using droplet digital PCR.Clin Cancer Res. 2015;21(15):3552–3560; doi: 10.1158/1078-0432.CCR-14-2151.
- Beck J, Bierau S, Balzer S, et al. Digital droplet PCR for rapid quantification of donor DNA in the circulation of transplant recipients as a potential universal biomarker of graft injury.Clin Chem. 2013;59(12):1732–1741; doi: 10.1373/clinchem.2013.210328.
- Whale AS, Devonshire AS, Karlin-Neumann G, et al. International interlaboratory digital PCR study demonstrating high reproducibility for the measurement of a rare sequence variant.Anal Chem. 2017;89(3):1724–1733; doi: 10.1021/acs.analchem.6b03980.
- Zhang BO, Xu CW, Shao Y, et al. Comparison of droplet digital PCR and conventional quantitative PCR for measuring EGFR gene mutation. Exp Ther Med. 2015;9(4):1383–1388; doi: 10.3892/etm.2015.2221.
- Beaver JA, Jelovac D, Balukrishna S, et al. Detection of cancer DNA in plasma of patients with early-stage breast cancer.Clin Cancer Res. 2014;20(10):2643–2650; doi: 10.1158/1078-0432.CCR-13-2933.
- Reid AL, Freeman JB, Millward M, Ziman M, Gray ES. Detection of BRAF-V600E and V600K in melanoma circulating tumor cells by droplet digital PCR.Clin Biochem. 2015;48(15):999–1002; doi: 10.1016/j.clinbiochem.2014.12.007.
- Sanmamed MF, Fernández-Landázuri S, Rodríguez C, et al. Quantitative cell-free circulating BRAF-V600E mutation analysis by use of droplet digital PCR in the follow-up of patients with melanoma being treated with BRAF inhibitors.Clin Chem. 2015;61(1):297–304; doi: 10.1373/clinchem.2014.230235.
- Mattingley J, Oettel K. Blood-based genomic and proteomic testing for newly diagnosed lung cancer patients to facilitate rapid treatment decisions and prognostic conversations.CHEST Annual Meeting Abstracts. 2016;150(4_S):721A; doi: 10.1016/j.chest.2016.08.816.
- Zhu G, Ye X, Dong Z, et al. Highly sensitive droplet digital PCR method for detection of EGFR-activating mutations in plasma cell-free DNA from patients with advanced non-small cell lung cancer.J Mol Diagn. 2015;17(3):265–272; doi: 10.1016/j.jmoldx.2015.01.004.
- Sacher AG, Paweletz C, Dahlberg SE, et al. Prospective validation of rapid plasma genotyping for the detection of EGFR and KRAS mutations in advanced lung cancer. JAMA Oncol. 2016;2(8):1014–1022; doi: 10.1001/jamaoncol.2016.0173.
- Karlin-Neumann G. Improved liquid biopsies with combined digital PCR and next-generation sequencing [online].Am Lab. February 19, 2016. Available at: www.americanlaboratory.com/914-application-notes/183421-improved-liquid-biopsies-with-combined-digital-pcr-and-next-generation-sequencing. Accessed April 30, 2017.
- Liquid biopsy researchers to share their strategies for pairing digital PCR and next-generation sequencing at precision medicine world conference [press release]. Hercules, Calif: Bio-Rad Laboratories, 2017. Available at: www.bio-rad.com/en-us/life-science-research/news/liquid-biopsy-researchers-to-share-their-strategies-for-pairing-digital-pcr-and-next-generation-sequencing-at-precision-medicine-world-conference. Accessed April 30, 2017.
- Mellert H, Foreman T, Jackson L, et al. Development and clinical utility of a blood-based test service for the rapid identification of actionable mutations in non-small cell lung carcinoma. J Mol Diagn. 2017;19(3):404–416; doi: 10.1016/j.jmoldx.2016.11.004.
- Topalian SL, Drake CG, Pardoll DM. Targeting the PD-1/B7-H1(PD-L1) pathway to activate antitumor immunity.Curr Opin Immunol. 2012;24(2):207–212; doi: 10.1016/j.coi.2011.12.009.



{kind=link}