This year’s flu season requires clinical labs to take into account a variety of new considerations, including FDA reclassification of RIDTs.
By Patrick Murray, PhD

Figure 1. Image of flu virus.
Vaccines are the best defense against influenza, but predicting when influenza will occur and which strains will appear is a challenge (see Figure 1). In 2009, a novel strain of influenza A arose during the summer, and continued with significant disease into the fall.1 In 2013, a new strain, H3N2, made its debut and was responsible for the majority of disease that year.1 This strain has been the predominant virus in seasonal outbreaks for the past 3 years. Despite the fact that this strain is covered under current vaccines and was once again responsible for the majority of influenza cases during the 2016–2017 flu season, however, the prevalence of the strain led to particularly severe outcomes for children and older adults.1
So far—as of the beginning of November—the 2017–2018 flu season has seen low activity across the United States. Where flu activity has been reported, influenza A is the predominant strain (see Figures 2, 3).1,2
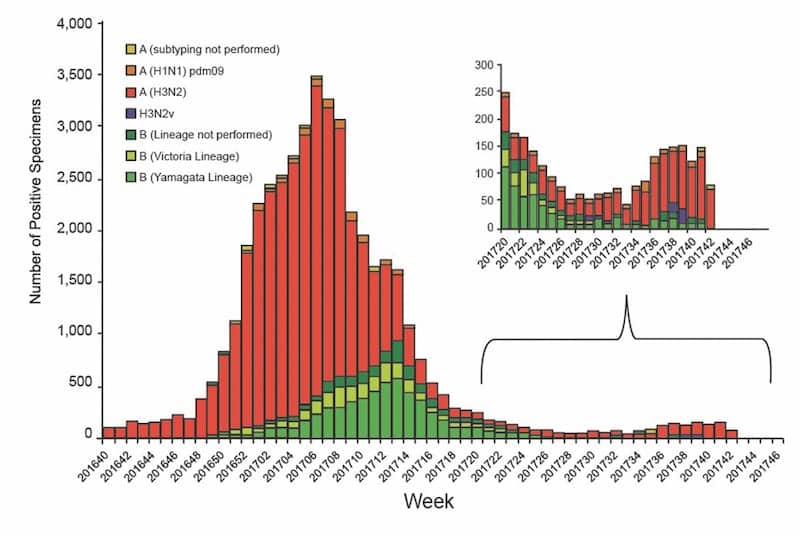
Figure 2. Influenza-positive tests reported to the Centers for Disease Control and Prevention by US public health laboratories, national summary, October 2, 2016–October 21, 2017.2 Click to expand.
In spite of efforts to predict which influenza strains will be most prevalent in a given year and to vaccinate as many people as possible, millions of people are still affected by the virus annually in the United States, hundreds of thousands are hospitalized, and thousands die.1 Historically, vaccination rates range from 32% to 67% depending on patient age, and vaccine effectiveness is only 50% to 60% due to new strains in the community, patient response to the vaccine, and virus factors (see Table 1).1–15 As influenza can rapidly mutate to avoid the host immune response, vaccine effectiveness can change from year to year even with similar strain coverage.3 The flu vaccine also doesn’t work the same for all people: it’s most effective in healthy adults, and as people age or develop chronic illnesses immunity may become weaker.1 There may also be differences in immunity depending on the vaccine type an individual receives.3
Given all these factors, testing for influenza is more important than ever to mitigate the impact of influenza on a population. Identifying who has the flu and being able to quickly detect the virus if those around them develop symptoms can help public health officials contain its spread. Labs at national, regional, state, and local levels play a critical role in this process. Clinical lab managers have an opportunity to consider how their labs can support this important work, and point-of-care (POC) flu tests are making it easier than ever to do so.
The Importance of POC Testing

Table 1. Adjusted vaccine effectiveness estimates for influenza seasons from 2005 through 2017.1,4 Click to expand.
Early detection of influenza can support decisions to implement infection control measures in order to reduce the spread of disease.1 Having the right tools to detect influenza is important, as distinguishing between influenza and other illnesses (eg, adenovirus, coronavirus, metapneumovirus, respiratory syncytial virus) can be challenging for healthcare providers. The clinical symptoms of such upper respiratory infections are often indistinguishable, and they may all be prevalent at the same time of year.16
Detecting influenza early is critical for treating the illness and its symptoms effectively, thereby helping prevent the spread of disease. But it’s also an essential component of efforts to slow the development of organisms with antimicrobial resistance. Getting the correct diagnosis at the point of care facilitates immediate and effective treatment for influenza (if needed, based on the provider’s clinical judgment), and naturally blocks the prescription of antibiotics to patients who are unlikely to benefit because their infections are viral in nature. In turn, this practice will prevent overuse of antibiotics, helping to limit the growth of antibiotic-resistant bacteria and reducing unnecessary ancillary testing.17 Central labs may play a part in the selection, adoption, and implementation of POC flu tests for affiliated clinics and urgent care settings, and may continue to do so with a focus on improving patient outcomes and reducing antimicrobial resistance.

Figure 3. Influenza-positive tests reported to the Centers for Disease Control and Prevention by US clinical laboratories, national summary, October 2, 2016–October 21, 2017.2 Click to expand.
Hospitals and laboratory networks are also pivotal in tracking influenza outbreaks and the epidemiology of the disease. The 2009 influenza season highlighted the important role that POC testing can have in influenza detection. That season posed special challenges for the healthcare community due to the emergence of the H1N1 strain during the spring of that year. H1N1 caused the first influenza pandemic in more than 40 years, and required patients to receive a second vaccine on top of the seasonal one. In addition, the pandemic highlighted the inadequate performance of the rapid influenza diagnostic tests (RIDTs) available at the time, and raised concerns regarding the accuracy of detecting influenza in patients.1
FDA Reclassification
FDA concerns about the sensitivity of antigen-based RIDTs following the 2009 influenza season led to an examination of the regulation of these devices by the agency’s microbiology device panel. The panel cited low sensitivity and the risk of false negatives among the reasons for its recommendation to reclassify the devices and impose special controls to ensure the safety and effectiveness of RIDTs.18,19
After a 4-year process, in January 2017 FDA finalized its decision to reclassify devices for detecting influenza viruses from Class I to Class II (with special controls) and to hold them to higher clinical performance requirements.18 This was the first significant change to the regulation of RIDTs since 1990, when the first RIDT for use with clinical specimens was approved as a Class I test. Unfortunately, many of the RIDTs produced during the intervening years had poor analytical and clinical sensitivity: the sensitivity of most of the first-generation RIDTs ranged from 40% to 70%.20
As part of its reclassification of RIDTs, FDA is raising the required performance of the tests (see “Higher Performance Standards“). Together with other performance requirements, the new performance standards will require a sensitivity of at least 90% for influenza A and 80% for influenza B when compared to viral culture testing, or a positive percent agreement of at least 80% for influenza A and B when compared to molecular diagnostics using polymerase chain reaction (PCR) methods.21,22
Bracing for Impact
With this reclassification, labs and other facilities performing POC testing will have to reexamine their POC testing strategy to ensure they are meeting the new guidelines. Two categories of testing to consider are the new generation of rapid influenza diagnostic devices—digital immunoassays and nucleic acid amplification tests.

Figure 4. The BD Veritor Flu A+B assay is a digital immunoassay performed on the Veritor Plus analyzer, using instrumented interpretation of test results to satisfy FDA’s new Class II requirements for rapid influenza diagnostic tests.
FDA-cleared digital immunoassay systems have significantly improved upon earlier RIDTs in sensitivity and specificity because new detection technologies, interpretive software, and instrumented interpretation of results improve both assay sensitivity and specificity (see Figure 4).23,24 Nucleic acid amplification assays are another alternative, but since they are costlier to run, their practical use in POC settings is still limited. Both digital immunoassays and nucleic acid amplification tests are sensitive during the acute presentation of disease when high virus levels are present in respiratory specimens.
Labs that are using a testing system that does not meet the new guidelines should know that each manufacturer of currently marketed devices subject to the reclassification is responsible for compliance with the new special controls and must, by 12 January 2018, cease distributing a product if the labeled claims on that product do not meet the new performance criteria. Customers may continue using any of those products that they have remaining in stock after that date.
Taking into account vaccination rates that do not meet the threshold for herd immunity and suboptimal vaccine effectiveness, lab managers may play a critical role in future influenza seasons as they prepare for changes to the industry, including FDA reclassification. Fortunately, there are RIDTs that will meet the needs of nimble, modern healthcare providers, and will help labs support the treatment of influenza and minimize its spread.
Patrick Murray, PhD, is senior director for worldwide scientific affairs at BD. For further information, contact CLP chief editor Steve Halasey via [email protected].
REFERENCES
- Influenza (flu) [online]. Atlanta: Centers for Disease Control and Prevention, 2017. Available at: www.cdc.gov/flu/index.htm. Accessed September 25, 2017.
- Weekly US influenza report: 2017–2018 influenza season week 42 ending October 21, 2017 [online]. Atlanta: Centers for Disease Control and Prevention, 2017. Available at: www.cdc.gov/flu/weekly/index.htm#S1. Accessed October 30, 2017.
- Jackson M, Chung J, Jackson L, et al. Influenza vaccine effectiveness in the United States during the 2015–2016 season. N Engl J Med. 2017;377(6):534–543; doi: 10.1056/nejmoa1700153.
- Seasonal influenza vaccine effectiveness, 2005–2017 [online]. Atlanta: Centers for Disease Control and Prevention, 2017. Available at: www.cdc.gov/flu/professionals/vaccination/effectiveness-studies.htm. Accessed October 25, 2017.
- Belongia EA, Kieke BA, Donahue JG, et al. Effectiveness of inactivated influenza vaccines varied substantially with antigenic match from the 2004–2005 season to the 2006–2007 season. J Infect Dis. 2009;199(2):159–167; doi:10.1086/595861.
- Belongia EA, Kieke BA, Donahue JG, et al. Influenza vaccine effectiveness in Wisconsin during the 2007–2008 season: comparison of interim and final results. Vaccine. 2011;29(38):6558-6563; doi: 10.1016/j.vaccine.2011.07.002.
- Griffin MR, Monto AS, Belongia EA, et al. Effectiveness of non-adjuvanted pandemic influenza A vaccines for preventing pandemic influenza acute respiratory illness visits in 4 US communities. PLoS One. 2011;6(8):e23085; doi: 10.1371/journal.pone.0023085.
- Treanor JJ, Talbot HK, Ohmit SE, et al. Effectiveness of seasonal influenza vaccines in the United States during a season with circulation of all three vaccine strains. Clin Infect Dis. 2012;55(7):951–959; doi: 10.1093/cid/cis574.
- Ohmit SE, Thompson MG, Petrie JG, et al. Influenza vaccine effectiveness in the 2011–2012 season: protection against each circulating virus and the effect of prior vaccination on estimates. Clin Infect Dis. 2014;58(3):319–327; doi: 10.1093/cid/cit736.
- McLean HQ, Thompson MG, Sundaram ME, et al. Influenza vaccine effectiveness in the United States during 2012–2013: variable protection by age and virus type. J Infect Dis. 2015;211(10):1529–1540; doi: 10.1093/infdis/jiu647.
- Gaglani M, Pruszynski J, Murthy K, et al. Influenza vaccine effectiveness against 2009 pandemic influenza A(H1N1) virus differed by vaccine type during 2013–2014 in the United States. J Infect Dis. 2016;213(10):1546–1556; doi: 10.1093/infdis/jiv577.
- Zimmerman RK, Nowalk MP, Chung J, et al. 2014–2015 influenza vaccine effectiveness in the United States by vaccine type. Clin Infect Dis. 2016;63(12):1564–1573; doi: 10.1093/cid/ci-w635.
- Jackson ML, Chung JR, Jackson LA, et al. Influenza vaccine effectiveness in the United States during the 2015–2016 season. N Engl J Med. 2017;377(6):534–543; doi: 10.1056/nejmoa1700153.
- Ferdinands J. Influenza vaccine effectiveness, 2016–2107; US flu VE network and US hospitalized adult influenza vaccine effectiveness network (HAIVEN) [online]. Presentation to a meeting of the Advisory Committee on Immunization Practices, Atlanta, National Center for Immunization and Respiratory Diseases, 21 June 2017. Available at: www.cdc.gov/vaccines/acip/meetings/downloads/slides-2017-06/flu-03-ferdinands.pdf. Accessed October 25, 2017.
- Update: influenza activity in the United States during the 2016–2017 season and composition of the 2017–2018 influenza vaccine. Morb Mortal Wkly Rep. 2017;66(25):668–676. Available at: www.cdc.gov/mmwr/volumes/66/wr/mm6625a3.htm?s_cid=mm6625a3_w. Accessed August 25, 2017.
- Zambon MC, Stockton JD, Clewley JP, Fleming DM. Contribution of influenza and respiratory syncytial virus to community cases of influenza-like illness: an observational study. Lancet. 2001;358(9291):1410–1416.
- Blaschke AJ, Shapiro DJ, Pavia AT, et al. A national study of the impact of rapid influenza testing on clinical care in the emergency department. J Pediatric Infect Dis Soc. 2013;3(2):112–118; doi: 10.1093/jpids/pit071.
- Microbiology devices; reclassification of influenza virus antigen detection test systems intended for use directly with clinical specimens [proposed rule]. 79 Federal Register 99 (May 22, 2014):29387–29392. Available at: www.gpo.gov/fdsys/pkg/FR-2014-05-22/pdf/2014-11635.pdf. Accessed October 25, 2017.
- 2013 Meeting Materials of the Microbiology Devices Panel [online]. Silver Spring, Md: FDA, 2013. Available at: https://wayback.archive-it.org/7993/20170405192834/https:/www.fda.gov/advisorycommittees/committeesmeetingmaterials/medicaldevices/medicaldevicesadvisorycommittee/microbiologydevicespanel/ucm356061.htm. Accessed July 28, 2017.
- Evaluation of rapid influenza diagnostic tests for detection of novel influenza A (H1N1) virus: United States, 2009. Morb Mortal Wkly Rep. 2009;58(30):826–829. Available at: www.cdc.gov/mmwr/preview/mmwrhtml/mm5830a2.htm. Accessed October 26, 2017.
- Microbiology devices; reclassification of influenza virus antigen detection test systems intended for use directly with clinical specimens [final rule]. 82 Federal Register 8 (January 12, 2017):3609–3619. Available at: www.federalregister.gov/documents/2017/01/12/2017-00199/microbiology-devices-reclassification-of-influenza-virus-antigen-detection-test-systems-intended-for. Accessed August 8, 2017.
- Merckx J, Wali R, Schiller I, et al. Diagnostic accuracy of novel and traditional rapid tests for influenza infection compared with reverse transcriptase polymerase chain reaction: a systematic review and meta-analysis. Ann Intern Med. 2017;167(6):394–409; doi: 10.7326/m17-0848.
- Hassan F, Nguyen A, Formanek A, Bell J, Selvarangan R. Comparison of the BD Veritor system for flu A+B with the Alere BinaxNow influenza A&B card for detection of influenza A and B viruses in respiratory specimens from pediatric patients. J Clin Microbiol. 2014;52(3):906–910; doi: 10.1128/jcm.02484-13.
- Dunn J, Obuekwe J, Baun T, Rogers J, Patel T, Snow L. Prompt detection of influenza A and B viruses using the BD Veritor system flu A+B, Quidel Sofia influenza A+B FIA, and Alere BinaxNow influenza A&B compared to real-time reverse transcription-polymerase chain reaction (RT-PCR). Diagn Microbiol Infect Dis. 2014;79(1):10–13; doi: 10.1016/j.diagmicrobio.2014.01.018.



{kind=link}