This is a companion article to the feature, “Training for Quality.”

W. Greg Miller, PhD, Virginia Commonwealth University.
To find out more about AACC’s continuing education program, “Practical Approaches to Quality Control in the Clinical Laboratory,” CLP recently spoke with W. Greg Miller, PhD, DABCC, professor of pathology at Virginia Commonwealth University, and program chair for the group of faculty and industry experts who created the individual courses of the program.
CLP: Have any of the techniques described in the program or in your own course been subject to recent updates as a result of revised regulations or standards?
Greg Miller, PhD: There have been a number of small updates. One of the more important clarifications was provided in the recently updated CLSI guideline, Statistical Quality Control for Quantitative Measurement Procedures: Principles and Definitions, and focuses on how laboratories should perform QC when changing reagent lots.1
Because of the way QC materials are manufactured, laboratories that change reagent lots can encounter a change in value for the QC result without any corresponding change in the value of a patient result (Figure 1). In such a situation, the lab needs to change the target value of its QC result and base its decision about whether the new reagent lot is acceptable on the patient results, which should be measured with both the old lot and the new lot.
CLP: What important technologies play a role in the techniques described in the program?
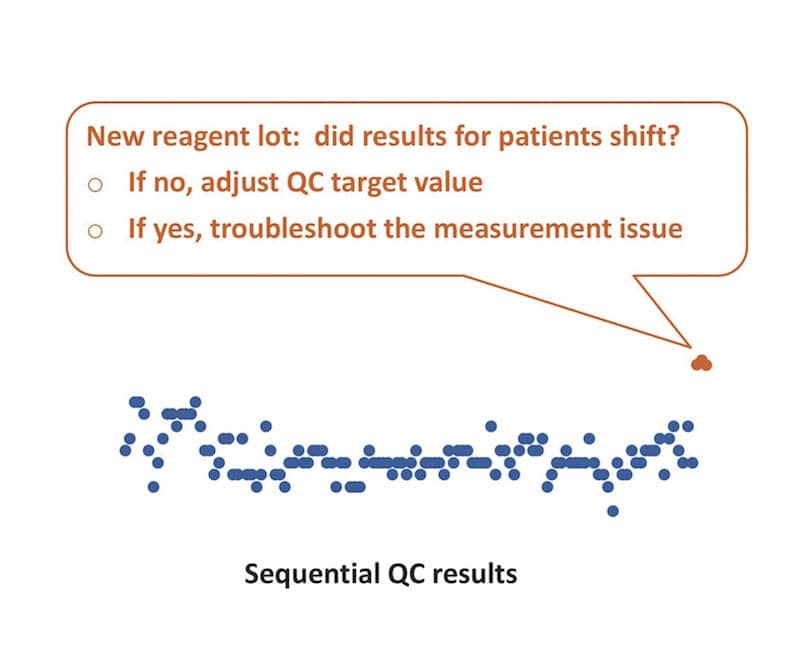
Figure 1. A QC program must recognize that reagent lot changes can affect QC results, even when patient test results remain unaffected.
Miller: In the context of this program, ‘controls’ are the liquid controls that simulate patient serum or urine specimens. Electronic systems are also important, because they validate that the measurement tool itself is working. Systems of this type are particularly important for instruments that are used in point-of-care settings.
Calibrators don’t play a direct role in QC testing, except that the laboratory must obviously calibrate its testing methods, and one of the purposes of QC is to determine that the lab’s calibration has remained stable. So calibrators are part of the measurement procedure, and controls are used to verify that the measurement procedure has remained stable.
CLP: How do these technologies help laboratorians perform the techniques described in the courses of this program, and what issues need to be watched for when using them?
Miller: The techniques described in the various courses are intended to provide laboratories with the basic tools needed to set up a rational QC program based on the performance characteristics of the measurement procedure they’re dealing with, and taking into account the risk of reporting an incorrect patient result that causes an unfavorable medical outcome.
The sequence of operations is to determine the number of controls that should be measured; determine how frequently to measure them; establish the target values and standard deviations representing the expected performance of the controls when the measurement system is working correctly; and create rules for evaluating how large a change in QC result is considered significant.
Developing follow-up activities is an important final step. Labs need to create a plan for what to do if they find a problem; they need to know how to stop processing new specimens; how to determine what the problem is; what corrective actions must be taken; and, most importantly, how to address the issue of any patient test results already reported when the QC system determined that there may have been a measurement problem.
So that’s the sequence of operations that a lab should apply when developing a QC program. But remember, before this program was created, people have been doing QC for a long time, so very little of this is new. What we think we’ve brought to the table is a very coherent, systematic strategy for setting up and using a QC system in the real world of a laboratory, and dealing with the problems that typical laboratories have to face.
CLP: I’ve sometimes heard laboratorians say that either they don’t feel comfortable relying on built-in electronic QC, or they don’t feel comfortable with reducing the number or frequency of QC runs based on the use of such tools. It sometimes isn’t clear whether the tools are more important than the techniques or the techniques are more important than the tools—or how they work together.
Miller: Some of this depends on the measurement system a lab is using. Some instruments have much more sophisticated built-in monitoring systems that act as controls—not liquid QC controls, but controls of the overall process. A laboratory that is using a device with a lot of built-in self-checking may have greater confidence that the device itself will identify an error condition when something needs to be fixed.
Instruments that incorporate sophisticated electronic controls can enable laboratories to monitor a lot of activities in real time. Using such systems, for instance, labs can monitor the magnitude of a test’s chemical reaction, the size of the test signal, or the stability of the entire platform. There are a lot of things that can be monitored using a modern measurement system.
One of the key points that our program brings up is the utility of such electronic controls for performing a risk-based assessment as the basis for setting up a QC program. This sort of functionality has only come about in the past 6 or 8 years, and it is entirely dependent on the availability of built-in electronic controls. Manufacturers are now building into their instruments robust management systems and stable measurement systems that can help laboratories determine how frequently they need to perform external QC using liquid controls.
But one size does not fit all. There’s no way to just say, ‘do this and you’ll be fine.’ Laboratories need to assess the overall set of tools available to them, and then determine how frequently they need to perform testing using a surrogate QC sample material. The entire certificate program is really built around that piece of the QC process. Everything else—all the other steps and procedures described in the courses—is just a matter of developing the methods needed to perform the actual QC testing process.
CLP: The program materials say specifically that the program does not cover development of an individualized quality control program (IQCP). Overall, does this course lead into the capabilities that labs need to create an IQCP, or is this something different altogether?
Miller: It’s something of a different animal. IQCP is really a process to evaluate the robustness of built-in control schemes and measurement procedures. The way IQCP is implemented is often a little bit formulaic, without necessarily thinking through all the ramifications of potential failure.
IQCP may be fine when a laboratory is using measurement devices with built-in controls that are sufficiently robust to make the probability of a failure extremely remote or, if a failure occurs, the worst outcome will be that the test result will not be available. In such cases, the risk of harm is very small, because if there’s a defect, the instrument simply won’t produce a result.
Many of the point-of-care devices that have evolved over the past 20 years or so have become extremely robust in this regard. They’re specifically engineered to be used outside the laboratory in a near-patient setting, and IQCP is really aimed at those types of devices.
The types of instruments that are used in the core chemistry lab environment today are certainly much more sophisticated than the instruments of 10 or 20 years ago. But labs must still rely very heavily on running QC materials on a scheduled basis, especially for continuous measurement systems, to determine whether the system is maintaining its stability. And that’s more the environment that our certificate program is aimed at: instruments used in the core lab setting that have fewer built-in failsafe systems than might be expected in a point-of-care device.
The certificate program is focused on instruments found in a typical core laboratory setting. But the principles also apply to point-of-care applications.
CLP: How do you hope that laboratorians will approach the course materials in order to get the most benefit from them?
Miller: Taken as a whole, the sequence of courses is designed to walk an individual through the different aspects of QC, and provide an understanding of what QC is supposed to do. But more than that, the courses explain how a laboratory can set up a QC system, how the system’s rules can be used to perform QC assessments, and what follow-up activities laboratories should be prepared to take in the event of a QC failure.
We end with a course on external quality assessment (EQA), which is a vital complement to a lab’s internal QC program that is often required by regulations. As with other sections of the program, we provide guidance about the best way to interpret the results of EQA, because such assessments have some characteristic limitations that laboratories need to understand.
Laboratorians will get a great deal from the how-to approach of the courses, but they should also pay attention to the sections in which methodological limitations and cautionary information are presented. We try to emphasize both aspects in each of the courses.
CLP: Overall, what is the value of a certificate program such as this for keeping laboratorians up to speed with practical instruction and essential lab techniques?
Miller: Laboratorians who spend the time to complete the program will end up with exactly the outcome you indicated: they will be up to speed with practical instruction in how to implement a QC plan. That’s the whole point of the program.
Obviously, there is a wide range of literature in this area, and laboratorians can deepen their understanding if they have the time to read lots of book chapters and articles that discuss the application of QC to clinical laboratory testing. But the advantage of the certificate program is that it offers commentary from experts who walk laboratorians through the slides that explain QC processes. So, laboratorians who simply view the slides and listen carefully will be guided through all the information needed to understand why QC is performed, how to set up a QC program, how to interpret the results, and how to follow up if a QC failure occurs.
The program is centered on the requirements for US laboratories, so the courses include a fair amount of material on documentation requirements to ensure that everything laboratories do is in conformity with the Clinical Laboratory Improvement Amendments of 1988 (CLIA). Elsewhere in the world, clinical laboratory accreditation typically follows the requirements of the standard on Medical Laboratories: Requirements for Quality and Competence(ISO 15189), compiled by the International Organization for Standardization.2 While the two regimes have different documentation requirements, they’re basically the same operationally; the way that a laboratory performs QC will be essentially the same under either of those two regulatory systems.
On the whole, the courses cover enough theory so that an individual can understand that the recommendations for how to implement QC are based on solid statistics and understandings of laboratory workflow. But the thrust of the program is still very pragmatically oriented. Participants will walk away with very practical knowledge about how to implement or tune up a QC program for their laboratories that represents the state of the art in terms of current practice.
References
- Statistical Quality Control for Quantitative Measurement Procedures: Principles and Definitions (CLSI Guideline C24), 4th ed. Wayne, Pa: Clinical and Laboratory Standards Institute, 2016. Available at: https://clsi.org/standards/products/clinical-chemistry-and-toxicology/documents/c24. Accessed April 30, 2018.
- Medical Laboratories: Requirements for Quality and Competence (ISO 15189:2012), 3rd ed. Geneva, Switzerland: International Organization for Standardization, 2012. Available at: www.iso.org/iso/catalogue_detail?csnumber=56115. Accessed April 28, 2018.



