AMH testing offers a measure of a woman’s ovarian reserve
By Michael Samoszuk, MD; Shamiram Feinglass, MD, MPH; and Lindsay (Xuan) Sun, MD
Measuring the levels of anti-Müllerian hormone (AMH) in the blood is an important means of answering a wide variety of questions relating to the reproductive system in women, men, and children. AMH assessment is important because of the high incidence of infertility or impaired fecundity in women. In this article, the authors review the biology and physiology of AMH and its relationship to fertility assessments in women.
The article also describes the technical features of various commercially available assays for measuring AMH, and compares the usefulness of measurements of AMH to measurements of follicle-stimulating hormone and other reproductive hormones. The clinical applications of AMH tests for assessment of fertility in women are discussed in detail, and the role of AMH in the assessment of other reproductive disorders—such as polycystic ovary syndrome and granulosa cell tumors—are briefly summarized.
Declining Fertility

Michael Samoszuk, MD, Beckman Coulter.
According to the Centers for Disease Control and Prevention, infertility and impaired fecundity are significant problems in the United States.1 Infertility is defined as the inability to become pregnant after 1 year of unprotected sex. Approximately 12% of women in the United States aged 15 to 44 have difficulty getting or staying pregnant.
The causes of infertility and impaired fecundity can be difficult to determine. About 30% of infertility cases can be attributed to specific causes in either the female or male; but 25% of such cases have no known cause.2 Infertility can have a profound impact on couples who wish to have children.
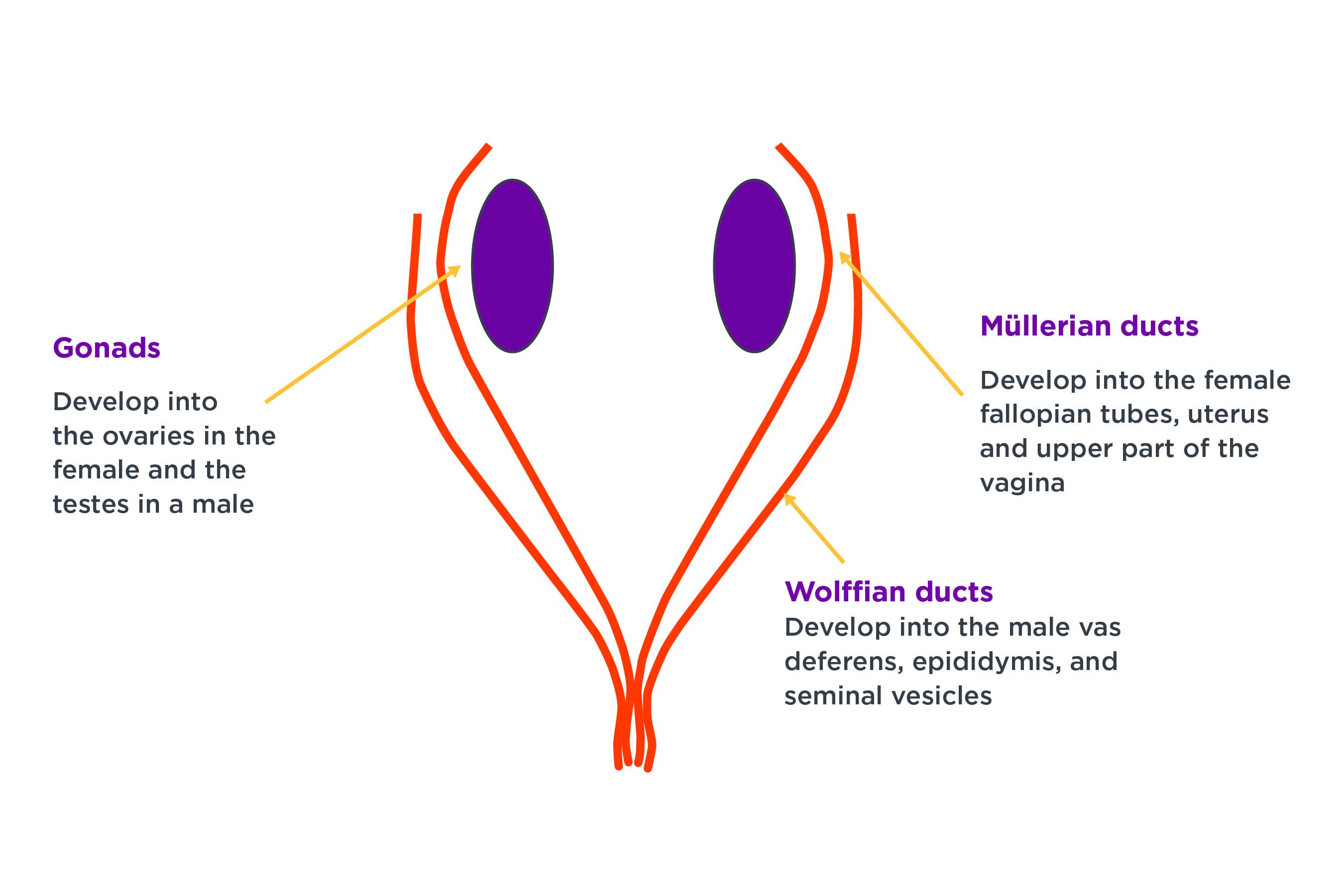
Figure 1. Embryology and anti-Müllerian hormone (AMH). During embryogenesis, AMH causes regression of the Müllerian ducts in males, permitting the Wolffian ducts to develop into the vas deferens, epididymis, and seminal vesicles. The absence of AMH in female embryos allows the Müllerian ducts to develop into fallopian tubes, the uterus, and the upper portion of the vagina.
Fertility in women is known to decline steadily with age.3 A factor that is closely related to fertility and aging in women is ‘ovarian reserve,’ a measure that reflects the number and quality of a woman’s available oocytes (eggs). Women are born with a limited number of eggs. The starting number is influenced by genetics and other environmental factors such as smoking or exposure to toxins.2,3 As women enter and proceed through their reproductive years, their number of available eggs begins to decline in an irreversible manner. For some women, there is a need for an accurate assessment of ovarian reserve.
The Biology and Physiology of AMH
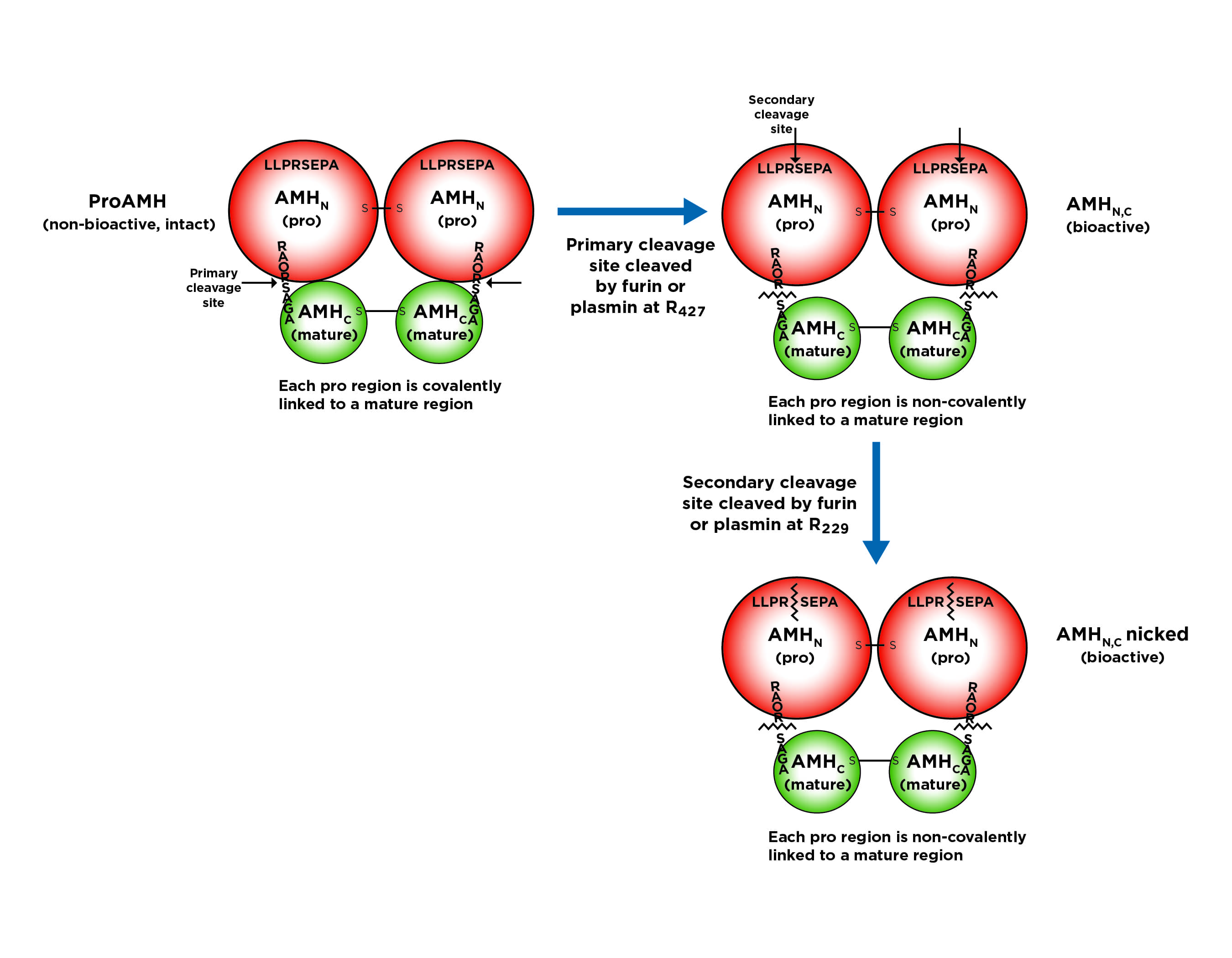
Figure 2. In blood, human anti-Müllerian hormone exists in three main structural forms: a non-bioactive, intact pro-form; and two bioactive forms that have undergone cleavage by furin or plasmin.
In males, AMH is produced by the Sertoli cells in the testicles. In females, it is produced by the granulosa cells of the follicles in the ovaries. AMH plays a number of roles over a person’s lifetime, and the quantity of AMH produced by an individual varies according to the individual’s sex and age.
During embryogenesis, AMH regulates sex differentiation. In male embryos, the presence of AMH causes regression of the Müllerian ducts, thereby permitting the Wolffian ducts to develop into the vas deferens, epididymis, and seminal vesicles (Figure 1).4 In female embryos, the absence of AMH allows the Müllerian ducts to develop into the fallopian tubes, the uterus, and the upper portion of the vagina.
In males, AMH regulates Leydig cell function in the testes, and Leydig cells synthesize testosterone. In females, the granulosa cells begin to produce AMH in late fetal life, and continue doing so until menopause. In adult women, AMH levels are a surrogate marker for the number of follicles in the ovary, where the eggs are contained.
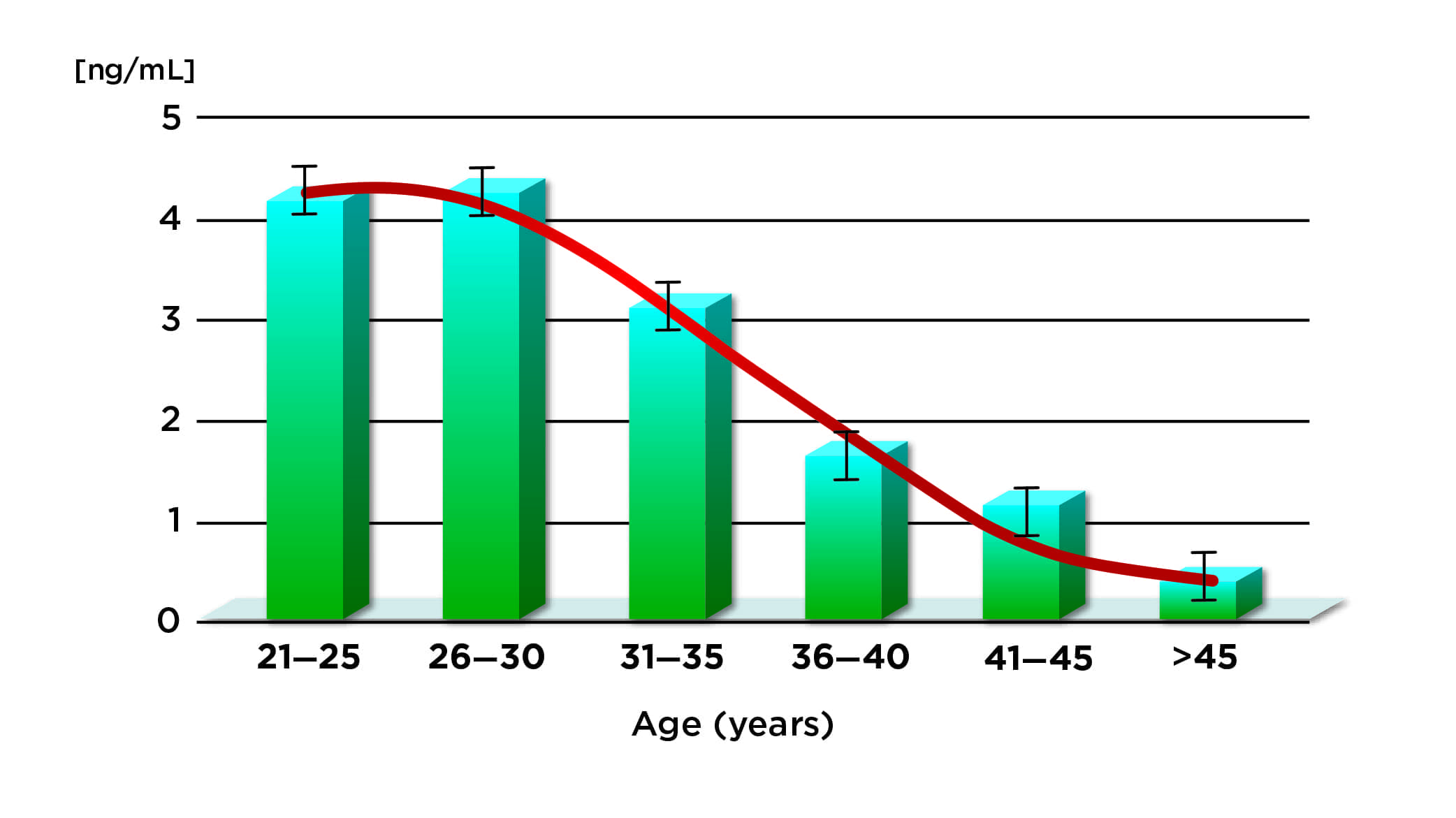
Figure 3. Age-related decline of anti-Müllerian hormone levels in women. Source: John K. Park, MD, MSc, Carolina Conceptions, Raleigh, NC.
In the blood, AMH exists in a non-bioactive, intact pro-form, and in two bioactive forms that have undergone cleavage by furin or plasmin.5 All three forms are recognized and can be measured by commercially available immunoassays such as the Access AMH assay by Beckman Coulter, Brea, Calif, and other immunoassays using the same AMH antibody pairs (Figure 2). Reflecting the age-related decline in a woman’s available eggs, the level of AMH shows a corresponding decline (Figure 3).6 The level of AMH remains fairly constant throughout the menstrual cycle; nevertheless, for purposes of standardization, manufacturers generally recommend sampling and testing on days 2?4 of the menstrual cycle.7
Tests for Measuring Ovarian Reserve
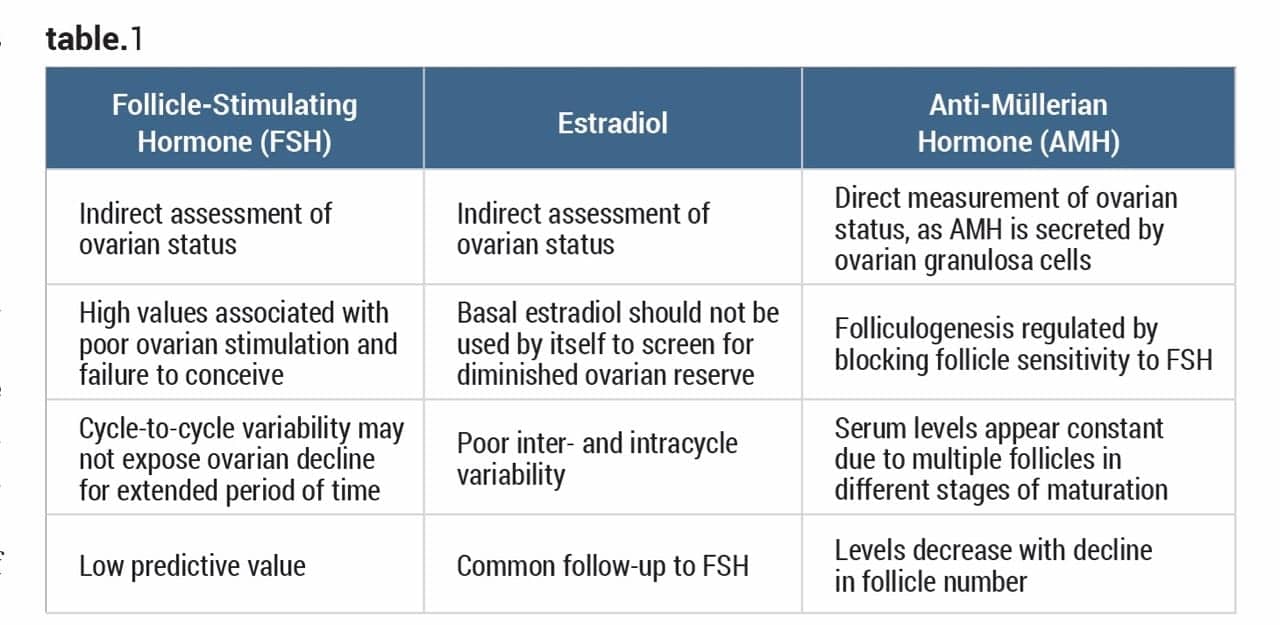
Table 1. Characteristics of endocrine assays commonly used to test for ovarian reserve.
To assess ovarian reserve, healthcare providers typically order a test for follicle-stimulating hormone (FSH), estradiol, or AMH (Table 1). Both FSH and estradiol provide indirect assessments of ovarian status and have a low predictive value. By contrast, AMH provides a direct measure of ovarian status, as it is secreted by the ovarian granulosa cells found in egg-bearing follicles. AMH levels decline as the number of follicles decreases.
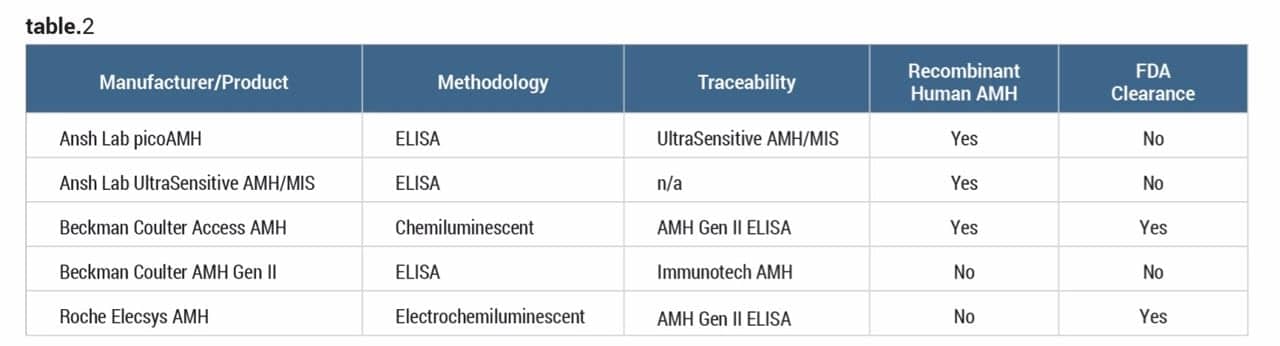
Table 2. Comparison of commercial anti-Müllerian hormone assays available in the United States. Source: product instructions for use.
A number of immunoassays for measuring AMH in blood are commercially available (Table 2). One notable difference among the various assays is that the Beckman Coulter automated product uses a human recombinant antigen as a calibrator. This method ensures greater consistency for the calibrator when compared to calibrators derived from bovine or other animal sources.
Ovarian reserve can also be assessed by ultrasound imaging of the ovaries, which permits counting of antral (small) follicles. The most accurate assessment of ovarian reserve is provided by ultrasound enumeration of antral follicles in conjunction with AMH tests.8 Indeed, there is a strong relationship between AMH levels and antral follicle count (AFC) as measured by ultrasound (Figure 4).9
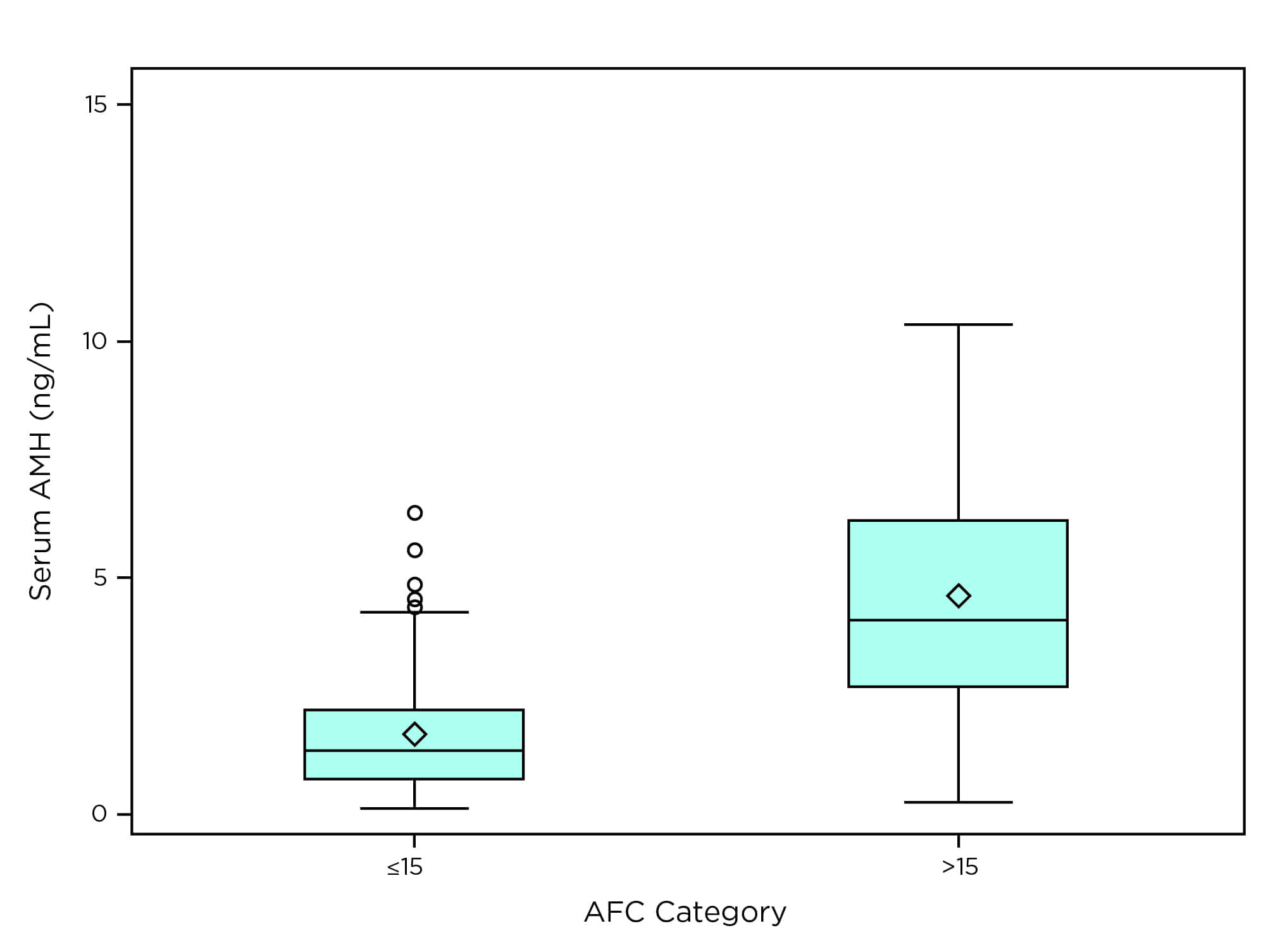
Figure 4. Box plot of the relationship between serum anti-Müllerian hormone (ng/mL) and antral follicle count categories. Source: Beckman Coulter Access AMH assay instructions for use.
An AMH value of 0 to 1.77 ng/mL is interpreted as normal to low. More than 90% of women with an AMH value in this range have an AFC less than or equal to 15. An AMH value greater than 1.77 ng/mL is interpreted as high, and corresponds to an AFC of greater than 15 in more than 50% of women. Nevertheless, it should be emphasized that neither AFC nor AMH levels directly indicate the probability of a woman becoming pregnant.
Other Clinical Applications of AMH
The earliest clinical investigations of AMH were for use in the evaluation of pediatric intersex disorders such as ambiguous genitalia.10 Undetectable AMH levels indicate the absence of testicular tissue. In males with precocious puberty (sexual maturity before the age of 9) AMH levels are abnormally low; whereas in males with delayed puberty, AMH levels are persistently high.11 AMH levels are detectable in cases of cryptorchidism (a condition in which one or both testes fail to descend normally), but undetectable in cases of anorchism (complete absence of one or both testes).

Shamiram Feinglass, MD, MPH, Beckman Coulter.
The AMH assay is used along with other reproductive testing to evaluate a woman’s ovarian reserve before starting fertility therapy with controlled ovarian stimulation (COS). If a woman has a very high AMH result, COS therapy will have a high probability of overstimulating the ovaries. The goal of COS is to ensure that a women ovulates with only a few eggs, but is not overstimulated to produce too many eggs, which can be dangerous. In the case of a high AMH test result, doctors can adjust the dosage of the fertility drugs, thereby reducing the likelihood of ovarian hyperstimulation syndrome.12
Another important application of the AMH assay is in reproductive aging research. AMH levels have been shown to be highly predictive for the age of onset of menopause.13 A related application is for fertility assessment in women before and after chemotherapy, which often induces premature menopause.14 This is an important consideration if fertility preservation is desired.
In men, AMH testing may have value for the assessment of hypogonadism (androgen deficiency) and infertility.15 There is evidence that men with reduced levels of testosterone have high levels of AMH. By contrast, in normal, healthy men, AMH levels remain low or undetectable.
Polycystic ovary syndrome (PCOS) affects up to 10% of the female population and is the most common cause of infertility due to anovulation.16 Patients typically present with virilization due to elevated androgen levels and polycystic ovaries on ultrasound examination. Polycystic ovaries lead to increased AMH levels, which then inhibit FSH, resulting in anovulation. Testing for AMH can therefore aid physicians in the evaluation of women suspected of having PCOS.17
Lindsay (Xuan) Sun, MD, Beckman Coulter.
Granulosa cell tumors comprise 2% to 5% of all ovarian tumors, and AMH is produced by granulosa cells.18 Multiple studies have demonstrated the value of AMH measurement in the diagnosis and monitoring of granulosa cell tumors.19–21 In one study, investigators also demonstrated a correlation between tumor mass and AMH level.22
Despite the promise of other clinical applications of AMH testing, such applications nevertheless remain investigational; they are not cleared by FDA for the US market.
Conclusion
Infertility is a significant healthcare concern worldwide, especially as older women attempt to get pregnant. AMH testing is a valuable tool for use in ovarian reserve evaluation and for controlled ovarian stimulation with in vitro fertilization.
Additional clinical applications for AMH testing go beyond fertility and include PCOS, granulosa cell tumors of the ovary, pediatric disorders, and assessment of infertility and hypogonadism in men.
Michael Samoszuk, MD, is a board-certified pathologist and chief medical officer; Shamiram Feinglass, MD, MPH, is a board-certified preventionist and leads global medical affairs; and Lindsay (Xuan) Sun, MD, is a senior scientific affairs manager; all are at Beckman Coulter. For further information, contact CLP chief editor Steve Halasey via [email protected].
References
- Reproductive health: infertility FAQs [online]. Atlanta: Centers for Disease Control and Prevention, 2018. Available at: www.cdc.gov/reproductivehealth/infertility/index.htm. Accessed May 15, 2018.
- Ghadir S, Ambartsumyan G, DeCherney AH. Infertility. Chapter 53 in: DeCherney AH, Nathan L, Laufer N, Roman AS, eds. Current Diagnosis & Treatment: Obstetrics & Gynecology. 11th ed. New York City: McGraw-Hill, 2013. Available at: http://accessmedicine.mhmedical.com/content.aspx?bookid=498§ionid=41008657. Accessed February 23, 2018.
- Evaluation of the infertile couple. In: Hoffman BL, Schorge JO, Bradshaw KD, Halvorson LM, Schaffer JI, Corton MM, eds. Williams Gynecology. 3rd ed. New York City: McGraw-Hill, 2016. Available at: http://accessmedicine.mhmedical.com/content.aspx?bookid=1758§ionid=118170398. Accessed February 23, 2018.
- Anawalt BD, Braunstein GD. Testes. In: Gardner DG, Shoback D, eds. Greenspan’s Basic & Clinical Endocrinology. 10th ed. New York City: McGraw-Hill, 2018. Available at: http://accessmedicine.mhmedical.com/content.aspx?bookid=2178§ionid=166250329. Accessed February 23, 2018.
- Pankhurst MW, McLennan IS. Human blood contains both the uncleaved precursor of anti-Müllerian hormone and a complex of the NH2- and COOH-terminal peptides. Am J Physiol Endocrinol Metab. 2013;305(10):E1241?E1247; doi: 10.1152/ajpendo.00395.2013.
- Plociennik L, Nelson SM, Lukaszuk A, et al. Age-related decline in AMH is assay-dependent, limiting clinical interpretation of repeat AMH measures across the reproductive lifespan. Gynecol Endocrinol. 2018;34(2):115?119; doi: 10.1080/09513590.2017.1358708.
- Rosen MP, Cedars MI. Female reproductive endocrinology and infertility. Chapter 13 in: Gardner DG, Shoback D, eds. Greenspan’s Basic & Clinical Endocrinology. 9th ed. New York City: McGraw-Hill, 2011. Available at: http://accessmedicine.mhmedical.com/content.aspx?bookid=380§ionid=39744053. Accessed February 23, 2018.
- Coelho Neto MA, Ludwin A, Borrell A, et al. Counting ovarian antral follicles by ultrasound: a practical guide. Ultrasound Obstet Gynecol. 2018;51(1):10?20; doi: 10.1002/uog.18945.
- Peres Fagundes PA, Chapon R, Olsen PR, Schuster AK, Mattia MMC, Cunha-Filho JS. Evaluation of three-dimensional Sono AVC ultrasound for antral follicle count in infertile women: its agreement with conventional two-dimensional ultrasound and serum levels of anti-Müllerian hormone. Reprod Biol Endocrinol. 2017;15(1):96; doi: 10.1186/s12958-017-0314-x.
- Lindhardt Johansen M, Hagen CP, Johannsen TH, et al. Anti-Müllerian hormone and its clinical use in pediatrics, with special emphasis on disorders of sex development. Int J Endocrinol. 2013;2013:198698; doi: 10.1155/2013/198698.
- Edelsztein NY, Grinspon RP, Schteingart HF, Rey RA. Anti-Müllerian hormone as a marker of steroid and gonadotropin action in the testis of children and adolescents with disorders of the gonadal axis. Int J Pediatr Endocrinol. 2016;2016:20; doi: 10.1186/s13633-016-0038-2.
- Styer AK, Gaskins AJ, Brady PC, et al. Dynamic anti-Müllerian hormone levels during controlled ovarian hyperstimulation predict in vitro fertilization response and pregnancy outcomes. Fertil Steril. 2015;104(5):1153?1161; doi: 10.1016/j.fertnstert.2015.07.1161.
- Kim C, Slaughter JC, Wang ET, et al. Anti-Müllerian hormone, follicle-stimulating hormone, antral follicle count, and risk of menopause within 5 years. Maturitas. 2017;102:18?25; doi: 10.1016/j.maturitas.2017.04.018.
- Anderson RA, Mansi J, Coleman RE, Adamson DJA, Leonard RCF. The utility of anti-Müllerian hormone in the diagnosis and prediction of loss of ovarian function following chemotherapy for early breast cancer. Eur J Cancer. 2017;87:58?64; doi: 10.1016/j.ejca.2017.10.001.
- Young J, Rey R, Couzinet B, Chanson P, Josso N, Schaison G. Anti-Müllerian hormone in patients with hypogonadotropic hypogonadism. J Clin Endocrinol Metab. 1999;84(8):2696?2699.
- Polycystic ovarian syndrome and hyperandrogenism. In: Hoffman BL, Schorge JO, Bradshaw KD, Halvorson LM, Schaffer JI, Corton MM, eds. Williams Gynecology. 3rd ed. New York City: McGraw-Hill, 2016. Available at: http://accessmedicine.mhmedical.com/content.aspx?bookid=1758§ionid=118170024. Accessed February 23, 2018.
- Ehrmann DA. Hirsutism. In: Kasper D, Fauci A, Hauser S, Longo D, Jameson J, Loscalzo J, eds. Harrison’s Principles of Internal Medicine. 19th ed. New York City: McGraw-Hill, 2014. Available at: http://accessmedicine.mhmedical.com/content.aspx?bookid=1130§ionid=79727043. Accessed February 23, 2018.
- Jeppesen JV, Anderson RA, Kelsey TW, et al. Which follicles make the most anti-Müllerian hormone in humans? Evidence for an abrupt decline in AMH production at the time of follicle selection. Mol Hum Reprod. 2013;19(8):519?27; doi: 10.1093/molehr/gat024.
- Haltia UM, Hallamaa M, Tapper J, et al. Roles of human epididymis protein 4, carbohydrate antigen 125, inhibin B, and anti-Müllerian hormone in the differential diagnosis and follow-up of ovarian granulosa cell tumors. Gynecol Oncol. 2017;144(1):83?89; doi: 10.1016/j.ygyno.2016.11.018.
- Färkkilä A, Koskela S, Bryk S, et al. The clinical utility of serum anti-Müllerian hormone in the follow-up of ovarian adult-type granulosa cell tumors: a comparative study with inhibin B. Int J Cancer. 2015;137(7):1661?1671; doi: 10.1002/ijc.29532.
- Färkkilä A, Haltia UM, Tapper J, McConechy MK, Huntsman DG, Heikinheimo M. Pathogenesis and treatment of adult-type granulosa cell tumor of the ovary. Ann Med. 2017;49(5):435?447; doi: 10.1080/07853890.2017.1294760.
- Chang HL, Pahlavan N, Halpern EF, MacLaughlin DT. Serum Müllerian-inhibiting substance/anti-Müllerian hormone levels in patients with adult granulosa cell tumors directly correlate with aggregate tumor mass as determined by pathology or radiology. Gynecol Oncol. 2009;114(1):57?60; doi: 10.1016/j.ygyno.2009.02.023.


{kind=link}
Great web site you have here.. It’s hard to find high-quality writing like yours these days. I truly appreciate individuals like you! Take care!!