
With syphilis rates on the rise, a reverse screening algorithm offers high clinical value
By Katherine Soreng, PhD
Syphilis is a systemic, sexually transmitted disease (STD) caused by the bacterium Treponema pallidum (subspecies pallidum).1,2 Despite efforts to eliminate the disease, healthcare statistics for the United States highlight a number of concerning trends in recent syphilis rates.

Katherine Soreng, PhD, Siemens Healthineers.
According to the US Centers for Disease Control and Prevention (CDC), rates of primary and secondary syphilis have risen nearly every year since 2001.3 The most recent available data (2015–2016) show that primary and secondary cases of syphilis have increased an alarming 14.7% among men and 35.7% among women.3 Rates of congenital syphilis have steadily increased since 2013, with a jump of 27.6% observed for 2015–2016.3 Men who have sex with men (MSM) continue to account for the majority of primary and secondary cases.3 However, during 2015–2016, rates increased among both men and women in every region of the United States. Pregnant women with syphilis are at elevated risk, due to poor outcomes associated with high vertical transmission rates and consequent fetal damage that can result in birth defects or loss of pregnancy.4
Effective treatment is available. T. pallidum has not demonstrated acquisition of significant antimicrobial resistance to penicillin, though resistance associated with alternative treatment regimens has been reported.4 Early detection and treatment are critical for reducing transmission and morbidity.3
Disease Progression and Transmission Risk
Untreated syphilis occurs in stages, typically beginning as a localized infection that subsequently spreads (Figure 1).5,6 Signs and symptoms related to primary and secondary syphilis may go unrecognized and can resolve without therapy, leading to disease progression.5 Latent disease is typically asymptomatic. Tertiary disease can be serious; complications include risk of severe cardiac or neurologic damage, or death.7,8
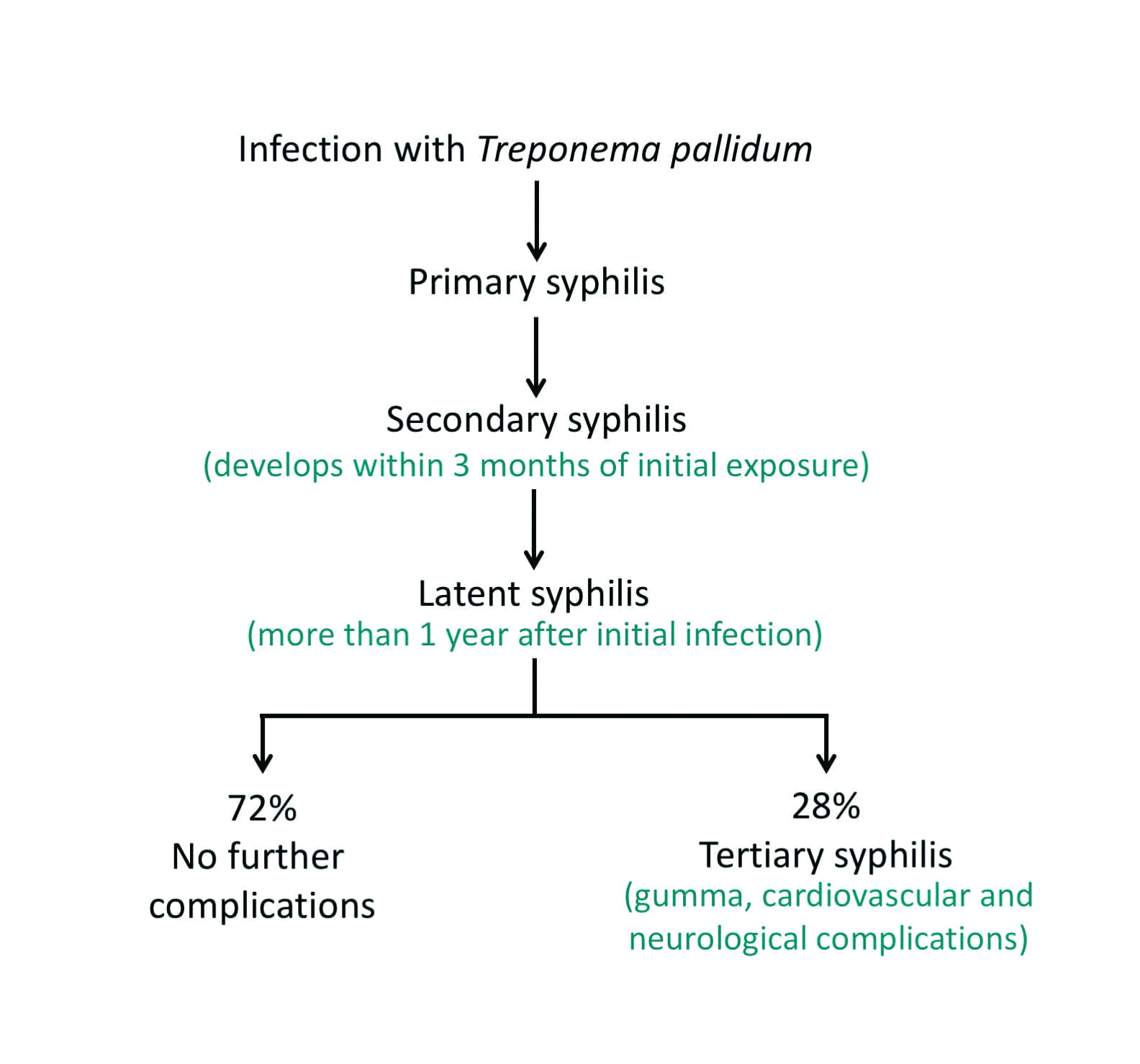
Figure 1. Course of untreated syphilis.1,36
Risk of transmission (both vertical and horizontal) is greatest during the primary and secondary stages. In utero transmission can occur during any stage—including the latent stage—though it is more likely to occur during the early stage than during the late-latent stage of the disease.5 Sequelae such as neurosyphilis and ocular syphilis can occur at any stage of disease and may result in severe complications, including blindness and death.5,6
Testing for Syphilis
Who Should Be Tested. Testing is recommended for those at risk, including patients with signs and symptoms, those engaging in high-risk behavior (such as MSM), and those infected with other STDs (including HIV).2,6
Testing of pregnant women is recommended regardless of risk.6,7 Pregnant women should be tested at their first prenatal visit, with subsequent testing indicated at the third trimester or at delivery for women at elevated risk or those residing in a community with high syphilis prevalence rates. All women who deliver a stillborn infant (after 20 weeks) should be tested for syphilis at the time of delivery.
Treatment for confirmed (or suspected) syphilis is highly efficacious. In pregnant women, treatment at least 30 days prior to delivery can prevent congenital infection, providing that grave infection of the fetus in utero has not already occurred.6 However, immunity does not accompany resolved infection, so repeat exposure can produce a new infection in need of treatment.
Syphilis Testing Options. Because T. pallidum cannot be cultured using traditional microbiological methods, testing for syphilis relies primarily on serology.9,10 Other techniques such as dark-field or fluorescent microscopy can be useful if a sample containing the treponemal organism is available (such as a lesion exudate or infected tissue), as the etiologic agent can be visualized.10,11
Molecular diagnostics using polymerase chain reaction (PCR) technologies have also been developed. A positive result from such a test can confirm the presence of treponemal DNA, but FDA has not approved any of the currently available molecular tests for syphilis screening.12 Most testing for a presumptive diagnosis of syphilis, including screening of pregnant women, relies on widely available and cost-effective serological assays.
A diagnosis of syphilis requires, at a minimum, the results of two types of serologic tests: nontreponemal and treponemal.9–13 While a single serological test—either nontreponemal or treponemal—can be useful for a rule-out, a rule-in requires results from both tests.
For many years, initial testing of patients for infection with T. pallidum has made use of nontreponemal assays such as the rapid plasma reagin (RPR) card or the Venereal Disease Research Laboratory (VDRL) test. The use of such nontreponemal tests for initial testing began when all available assays were manual and this option represented the most efficient approach. However, nontreponemal tests are known to be less clinically sensitive than other types of tests, and the wide availability of sensitive, automated treponemal immunoassays has challenged the earlier approach.
Nontreponemal tests recognize antibodies to lipoidal and other antigens released as a result of damage mediated by an infecting agent.14 However, many conditions not associated with T. pallidum infection can cause nontreponemal test reactivity, including acute viral infections, autoimmune disease, collagen disorders, and even pregnancy. So while nontreponemal assays are useful for identifying ongoing damage, they are not specific for syphilis.9,14
Nontreponemal tests can be run qualitatively or quantitatively. Quantitative tests (running at different dilutions of sample) can be useful in both confirmation and assessment of therapeutic response. Unlike treponemal antibodies, nontreponemal antibodies decrease and become undetectable with successful therapy.15,16 Some patients, especially those with repeat treponemal infection, may maintain a low level of nontreponemal reactivity (a serofast state).17 Additionally, up to 30% of untreated individuals with late-latent disease may seroconvert to nonreactivity for nontreponemal antibody.18–20
Treponemal assays recognize antibodies to one or more treponemal antigens—Tp15, Tp17, or Tp47—and are therefore more specific for treponemal infection.9,11,13 Establishing the presence of infection with the treponemal bacterium can thus be readily carried out by using such manual treponemal assays as T. pallidum particle agglutination (TP-PA) assays, fluorescent treponemal antibody absorbed (FTA-ABS) assays, or enzyme immunoassays; or by using automated chemiluminescent immunoassays.9 Although signs, symptoms, risk, and patient history need to be considered to make a diagnosis, reactivity in both treponemal and nontreponemal assays is consistent with syphilis infection in need of treatment.9
Treponemal assays are qualitative, and will detect the treponemal antibodies that tend to be present for life following seroconversion (and are present in both successfully treated and untreated patients).15 While treponemal assays thus have limited utility for identifying repeat infection, they are extremely useful for identifying initial infection, especially in low-prevalence populations (which generally include pregnant women).
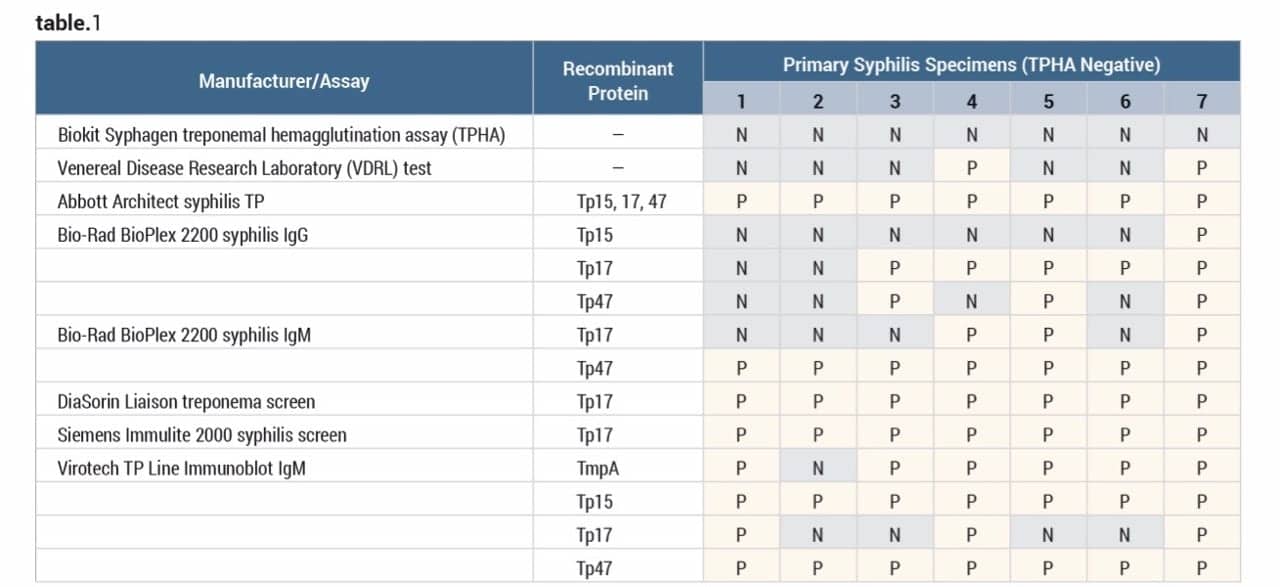
Table 1. Performance of five automated treponemal immunoassays from Abbott, Bio-Rad, DiaSorin, and Siemens on seven primary syphilis (TPHA-negative) specimens. Whenever an assay scored reactive, Line Immunoblot testing was used for confirmation. N = negative; P = positive. Adapted from Ly TD.22
Study data suggest that nontreponemal assays are less sensitive than many of the newer treponemal assays, especially for primary infection (Table 1). CDC reports that in primary syphilis, nontreponemal serologic tests are only about 75% sensitive.5 For both nontreponemal and treponemal assays, low assay sensitivity and the ‘window’ prior to seroconversion can contribute to missed primary infections.
CDC also warns of a ‘prozone effect’ in primary and secondary syphilis—that is, a false-negative test result that occurs when high antibody titers prevent antibody-antigen lattice formation.6 Such a prozone effect can occur with both nontreponemal and treponemal testing. Data about this phenomenon can generally be found in the manufacturer’s instructions for use or the assay package insert.
Evolving Algorithms
Traditional and Reverse Testing. In the early years of syphilis testing, both nontreponemal and treponemal assays were performed manually, and the nontreponemal assay (often the RPR test) was used for the initial screen.9 Reactive results were reflexed to a treponemal assay. This traditional approach was used as the standard screening algorithm for syphilis for many years.
With the advent of newer and more sensitive automated treponemal assays, however, many labs have opted to automate the initial screen by testing first with a treponemal assay, followed by testing reactive samples with a nontreponemal assay. This approach has been referred to as the ‘reverse screening algorithm.’9
When using the reverse screening algorithm, if the treponemal test is negative and consistent with the clinical picture, the patient can be ruled-out for infection. However, reactive treponemal test results must be followed by testing with a nontreponemal assay such as the RPR test. RPR and other nontreponemal tests—including quantitative RPR tests—therefore remain an important part of the diagnostic process.
Nontreponemal and treponemal assays are companion tests in the diagnosis of syphilis. The reverse algorithm changes the order of testing, using the treponemal assay first, but does not negate the value of nontreponemal tests. The value of adopting a reverse algorithm includes both clinical and workflow benefits.
Clinical Benefits of the Reverse Algorithm. One clinical advantage of adopting a reverse screening algorithm is the enhanced detection of late-latent syphilis cases that would go undetected using a traditional screening algorithm. Up to 30% of infected patients who progress to late-latent disease have negative results with nontreponemal tests, meaning that they could be missed if using a traditional algorithm.18–21
In cases of early (primary) syphilis, newer treponemal tests may also show increased sensitivity compared to nontreponemal tests, especially if they detect both IgG and IgM antibodies.13,22,23 Earlier detection can be especially important for reducing horizontal infection of sexual partners, and for initiating early treatment of pregnant women to minimize congenital syphilis. Although confirmation algorithms can differ, reverse screening is common and even recommended in many European countries.24
In a 2008 evaluation of data from four New York labs adopting a reverse algorithm approach, CDC noted the potential for the method to detect previously untreated syphilis at a higher frequency (though the data could not differentiate between treated and untreated patients).18 Additional studies have supported this observation.19,20 CDC encouraged clinicians to consider treatment of late-latent syphilis when treponemal testing results are reactive—even if active infection is not confirmed by a nontreponemal assay—in order to avoid the significant complications of tertiary disease. At the time of the New York study, CDC maintained its recommendation that labs continue using the traditional testing algorithm—but that recommendation is no longer current.
Current CDC Guidance
In the decade since the New York study, CDC’s guidance on syphilis testing has evolved from its previous support for traditional testing alone to the new position of supporting both the traditional and reverse screening algorithms.9 In its most recent guidance, CDC neutrally endorses both the traditional and reverse screening algorithms.
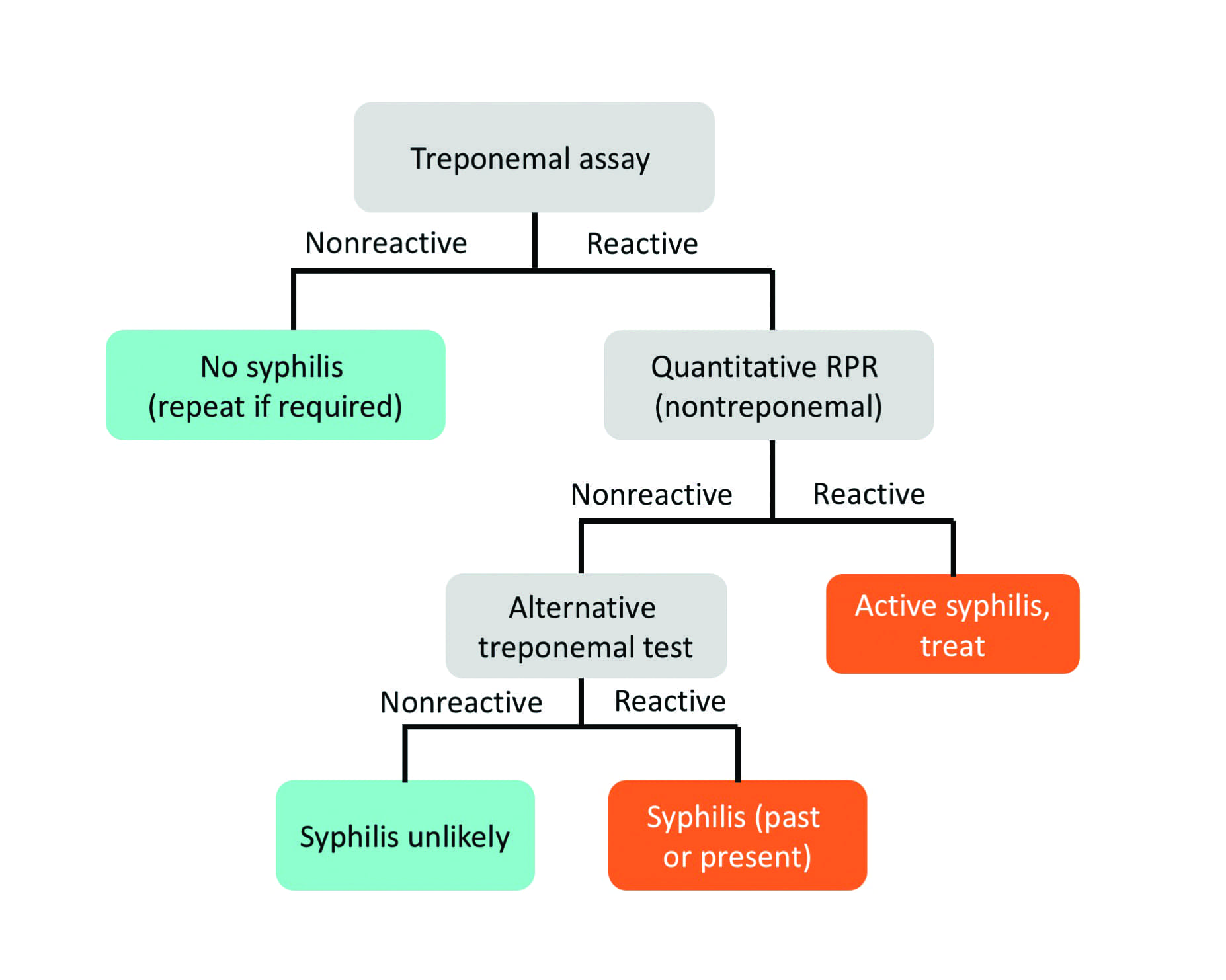
Figure 2. Designated algorithm from the Association of Public Health Laboratories and the US Centers for Disease Control and Prevention for a reverse approach to testing for syphilis.25
An informational brochure available from the Association of Public Health Laboratories (APHL) describes the traditional and reverse algorithms, interpretation of results, and suggested reporting language (Figure 2).9 In the case of discordant test results—samples reactive by treponemal testing and nonreactive by nontreponemal testing—APHL recommends that a second treponemal test (different from the screening test) be used to resolve the conflict. Reactivity of the second treponemal assay confirms the reactivity of the screening assay, and suggests the presence of a current or previous infection. Nonreactivity of the second treponemal assay suggests a potential false-positive screening result, though assessment of the clinical picture is important to rule-out infection.
Although CDC previously recommended the use of a TP-PA assay for the second, confirmatory test, the agency’s most recent guidance permits the use of alternative treponemal tests—with preference given to a test using different antigens from those used in the first test.9,25 Alternatives include TP-PA and other manual tests, such as FTA-ABS, as well as enzyme-linked immunosorbent assays (ELISAs) and automated immunoassays. The use of a second treponemal test aids in differentiating false-positive screening results from accurate screening results.
Discordant results can be associated with an early (primary) infection, late-latent disease, or previously resolved syphilis. For such cases, it is important that the clinician carefully review the patient’s medical history and consider the need to treat.
False-Positive and Discordant Results
Any assay has the potential for producing either a false-positive or false-negative result. RPR and other nontreponemal assays are subject to false-positive results because of the many conditions that damage human cells and cause the release of nontreponemal antigens, including acute viral infections and autoimmune disease.26,27 In such cases, the analytic result is valid, but represents a false-positive result for syphilis. Recent immunizations may also produce a transient presence of such antilipoidal antibodies. Analytic false positives (and false negatives) may also occur.
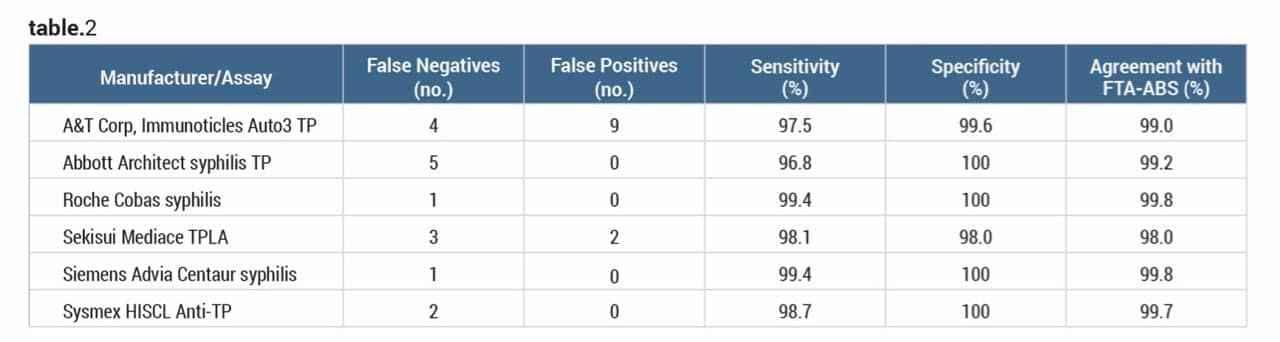
Table 2. Sensitivity and missed infection: performance of six commercial syphilis assays. Syphilis-positive results = 157 (155 patients, 2 standards). Adapted from Park BG.32
Treponemal testing—including testing in pregnant women—can also result in false-positive results.12,14,28 The use of a second treponemal test is highly useful for resolving discordant serology, and is the method currently recommended to differentiate results.
A recent CDC study explored the possibility of using immunoassay signal strength values (index or signal/cutoff) in lieu of confirmatory testing.29 Although the study data are not conclusive, they suggest that use of a defined, assay-specific cutpoint could reduce the need for confirmatory testing with a second treponemal assay.
Finally, while treponemal assays generally show good agreement, both false-positive and false-negative discrepancies have been reported—even among the newer automated assays.30–35 A recent study compared performance data from six commercially available treponemal assays (Table 2). Differences in test design may account in part for the discordance among the tests, and highlight the need for both high sensitivity and specificity when testing for syphilis.
Conclusion
The evolution of testing options for syphilis now allows for sensitive and early detection. Adoption of a reverse algorithm can improve both clinical detection and workflow, if the lab is using a sensitive, automated treponemal test.
CDC neutrally supports both traditional and reverse testing algorithms for syphilis. Adoption of an automated treponemal screening method offers significant advantages, especially for labs with high sample volumes that are testing primarily in a low-prevalence population, as compared to a higher prevalence setting such as an STD clinic.
Katherine Soreng, PhD, is director of clinical and scientific marketing at Siemens Healthineers. For more information, contact CLP chief editor Steve Halasey via [email protected].
References
- Lafond RE, Lukehart SA. Biological basis for syphilis. Clin Microbiol Rev. 2006;19(1):29–49; doi: 10.1128/cmr.19.1.29-49.2006.
- Bibbins-Domingo K, Grossman DC, Curry SJ, et al. Screening for syphilis infection in nonpregnant adults and adolescents: US Preventive Services Task Force recommendation statement. JAMA. 2016;315(21):2321?2327; doi: 10.1001/jama.2016.5824.
- Sexually transmitted disease surveillance, 2016 [online]. Atlanta: Centers for Disease Control and Prevention, 2017. Available at: www.cdc.gov/std/stats. Accessed April 13, 2018.
- Hawkes S, Matin N, Broutet N, Low N. Effectiveness of interventions to improve screening for syphilis in pregnancy: a systematic review and meta-analysis. Lancet Infect Dis. 2011;11(9):684?691; doi: 10.1016/s1473-3099(11)70104-9.
- Singh AE, Romanowski B. Syphilis: review with emphasis on clinical, epidemiologic, and some biologic features. Clin Microbiol Rev. 1999;12(2):187?209.
- Syphilis: pocket guide for providers. Atlanta: Centers for Disease Control and Prevention, 2017. Available at: www.cdc.gov/std/syphilis/syphilis-pocket-guide-final-508.pdf. Accessed April 13, 2018.
- Calonge N, Petitti DB, DeWitt TG, et al. Screening for syphilis infection in pregnancy: US Preventive Services Task Force reaffirmation recommendation statement. Ann Intern Med. 2009;150(10):705?709.
- Self-study STD modules for clinicians: syphilis. Atlanta: Centers for Disease Control and Prevention, 2017 [online]. Available at: http://www2a.cdc.gov/stdtraining/self-study/syphilis/default.htm. Accessed May 11, 2018.
- Suggested reporting language for syphilis serology testing. Silver Spring, Md: Association of Public Health Laboratories, 2015. Available at: www.aphl.org/aboutaphl/publications/documents/id_suggested_syphilis_reporting_lang_122015.pdf. Accessed March 30, 2018.
- Binnicker MJ. Which algorithm should be used to screen for syphilis? Curr Opin Infect Dis. 2012;25(1):79?85; doi: 10.1097/qco.0b013e32834e9a3c.
- Larsen SA, Steiner BM, Rudolph AH. Laboratory diagnosis and interpretation of tests for syphilis. Clin Microbiol Rev. 1995;8(1):1?21.
- Soreng K, Levy R, Fakile Y. Serologic testing for syphilis: benefits and challenges of a reverse algorithm. Clin Microbiol Newsl. 2014;36(24):195?202; doi: 10.1016/j.clinmicnews.2014.12.001.
- Sena AC, White BL, Sparling PF. Novel Treponema pallidumserologic tests: a paradigm shift in syphilis screening for the 21st century. Clin Infect Dis. 2010;51(6):700?708; doi: 10.1086/655832.
- Geusau A, Kittler H, Hein U, Dangl-Erlach E, Stingl G, Tschachler E. Biological false-positive tests comprise a high proportion of Venereal Disease Research Laboratory reactions in an analysis of 300,000 sera. Int J STD AIDS. 2005;16(11):722?726; doi: 10.1258/095646205774763207.
- Peeling RW, Ye H. Diagnostic tools for preventing and managing maternal and congenital syphilis: an overview. Bull World Health Organ. 2004;82(6):439?446.
- Larsen SA, Creighton ET. Rapid plasma reagin (RPR) 18-mm circle card test. In: Larsen SA, Pope V, Johnson RE, Kennedy EJ Jr, eds. A Manual of Tests for Syphilis. 9th ed. Atlanta: Centers for Disease Control and Prevention, 1998.
- Workowski KA, Berman S. Sexually transmitted diseases treatment guidelines, 2010. MMWR Recomm Rep. 2010;59(RR-12):1?110.
- Syphilis testing algorithms using treponemal tests for initial screening—four laboratories, New York City, 2005—2006. Morb Mortal Wkly Rep. 2008;57(32):872?875.
- Mishra S, Boily MC, Ng V, et al. The laboratory impact of changing syphilis screening from the rapid-plasma reagin to a treponemal enzyme immunoassay: a case-study from the Greater Toronto Area. Sex Transm Dis. 2011;38(3):190?196; doi: 10.1097/OLQ.0b013e3181f07e91.
- Singh AE, Wong T, De P. Characteristics of primary and late latent syphilis cases which were initially non-reactive with the rapid plasma reagin as the screening test. Int J STD AIDS. 2008;19(7):464?468; doi: 10.1258/ijsa.2007.007302.
- Jun L, He-Yi Z. Characteristics of patients with primary and late latent syphilis patients who were initially non-reactive to the rapid plasma reagin test. Jpn J Infect Dis. 2013;66(1):36?40.
- Ly TD, Marcenaro C, Dautigny M. Evaluation of four fully automated immunoassays for diagnosis of syphilis [abstract]. Poster P618, presented at the European Congress of Clinical Microbiology and Infectious Diseases, Vienna, April 10–13, 2010. Clin Microbiol Infect.2010;16(s2):S147. Available at: www.blackwellpublishing.com/eccmid20/PDFs/eccmid20_posters.pdf. Accessed May 17, 2018. ?
- Sednaoui P, Monfort L, Broyon J, Goubard A. Evaluation of the Advia Centaur syphilis assay in routine conditions for the diagnosis of syphilis [abstract and ePoster]. Poster P1748, presented at the European Congress of Clinical Microbiology and Infectious Diseases, Berlin, April 27–30, 2013. Available at: www.escmid.org/escmid_publications/escmid_elibrary/?q=Sednaoui&id=2173&L=0&tx_solr%5Bfilter%5D%5B0%5D=main_filter_eccmid%253Atrue&tx_solr%5Bfilter%5D%5B1%5D=pub_date%253A201301010000-201312312359&x=22&y=19. Accessed May 17, 2018.
- Janier M, Hegyi V, Dupin N, et al. 2014 European guideline on the management of syphilis. J Eur Acad Dermatol Venereol. 2014;28(12):1581?1593; doi: 10.1111/jdv.12734.
- Workowski KA, Bolan GA. Sexually transmitted diseases treatment guidelines, 2015. MMWR Recomm Rep. 2015;64(RR-03):1?137.
- Nandwani R, Evans DT. Are you sure it’s syphilis? A review of false-positive serology. Int J STD AIDS. 1995;6(4):241?248.
- Ratnam S. The laboratory diagnosis of syphilis. Can J Infect Dis Med Microbiol. 2005;16(1):45?51.
- Mmeje O, Chow JM, Davidson L, Shieh J, Schapiro JM, Park IU. Discordant syphilis immunoassays in pregnancy: perinatal outcomes and implications for clinical management. Clin Infect Dis. 2015;61(7):1049?1053; doi: 10.1093/cid/civ445.
- Fakile YF, Jost H, Hoover KW, et al. Correlation of treponemal immunoassay signal strength values with reactivity of confirmatory treponemal testing. J Clin Microbiol. 2017;56(1); doi: 10.1128/jcm.01165-17.
- Jonckheere S, Berth M, Van Esbroeck M, Blomme S, Lagrou K, Padalko E. Evaluation of different confirmatory algorithms using seven treponemal tests on Architect Syphilis TP-positive/RPR-negative sera. Eur J Clin Microbiol Infect Dis. 2015;34(10):2041?2048; doi: 10.1007/s10096-015-2449-z.
- Malm K, Andersson S, Fredlund H, et al. Analytical evaluation of nine serological assays for diagnosis of syphilis. J Eur Acad Dermatol Venereol. 2015;29(12):2369?2376; doi: 10.1111/jdv.13237.
- Park BG, Yoon JG, Rim JH, Lee A, Kim HS. Comparison of six automated treponema-specific antibody assays. J Clin Microbiol. 2016;54(1):163?167; doi: 10.1128/jcm.02593-15.
- Donkers A, Levy HR, Letens-van Vliet A. Syphilis detection using the Siemens Advia Centaur syphilis treponemal assay. Clin Chim Acta. 2014;433:84?87; doi: 10.1016/j.cca.2014.01.041.
- Jost H, Castro A, Cox D, et al. A comparison of the analytical level of agreement of nine treponemal assays for syphilis and possible implications for screening algorithms. BMJ Open. 2013;3(9):e003347; doi: 10.1136/bmjopen-2013-003347.
- Shieh JS, Stanley M, Bal T, Nabeck U. Syphilis testing: an automated immunoassay method-comparison study [abstract]. Poster D-90, presented at the annual meeting of the American Association for Clinical Chemistry, Atlanta, July 24–28, 2011. Clin Chem. 2011;57(S10):A162. Available at: www.aacc.org/science-and-practice/annual-meeting-abstracts-archive. Accessed May 18, 2018.
- Syphilis: CDC fact sheet (detailed) [online]. Atlanta: Centers for Disease Control and Prevention, 2017. Available at: www.cdc.gov/std/syphilis/STDFact-Syphilis-detailed.htm. Accessed May 4, 2018.



{kind=link}