Advanced testing methods promise improved patient outcomes and better protection of public health—with potential cost savings
By Erik Munson, PhD
Trichomoniasis is a sexually transmitted infection (STI) caused by the parasite Trichomonas vaginalis. It is the third-most prevalent STI in the United States—after human papilloma virus and herpes simplex virus infections—and the most prevalent nonviral STI.
The prevalence of trichomoniasis has been underestimated for several reasons: testing is not routinely undertaken among the asymptomatic patients who comprise roughly 80% of all cases; the most widely used diagnostic tools are relatively insensitive; and cases that are diagnosed are often not reported because there is no legal requirement to do so.
Undetected and therefore untreated trichomoniasis infections are associated with an increased occurrence of pregnancy complications, such as low birth weight and premature delivery, and with an increased risk and severity of certain other STIs (eg, HIV). Moreover, underreporting means that health systems do not have the data needed to develop strategies for protecting public health or informing resource allocation decisions.

Erik Munson, PhD, Marquette University.
New molecular technologies have the potential to shift the paradigm of how clinicians detect STIs such as trichomoniasis. Among these, nucleic acid amplification tests have emerged as a more reliable method of detecting T. vaginalis when compared with standard wet mount and culture tests. Improving diagnosis through the routine use of such molecular diagnostics would promote better health outcomes for patients who might otherwise go undiagnosed, and would provide more-accurate prevalence estimates to inform health system decisionmaking. In turn, more-accurate prevalence estimates might support mandatory reporting of trichomoniasis cases, enabling policymakers to better gauge and address the public health implications of this infection.
This article discusses the health implications of trichomoniasis and the challenges involved in diagnosing T. vaginalis infection, and describes the potential advantages for individual patients and the public health benefits of widespread use of nucleic acid amplification testing for this purpose. Potential cost advantages of universal T. vaginalis testing using a nucleic acid amplification platform will also be considered.
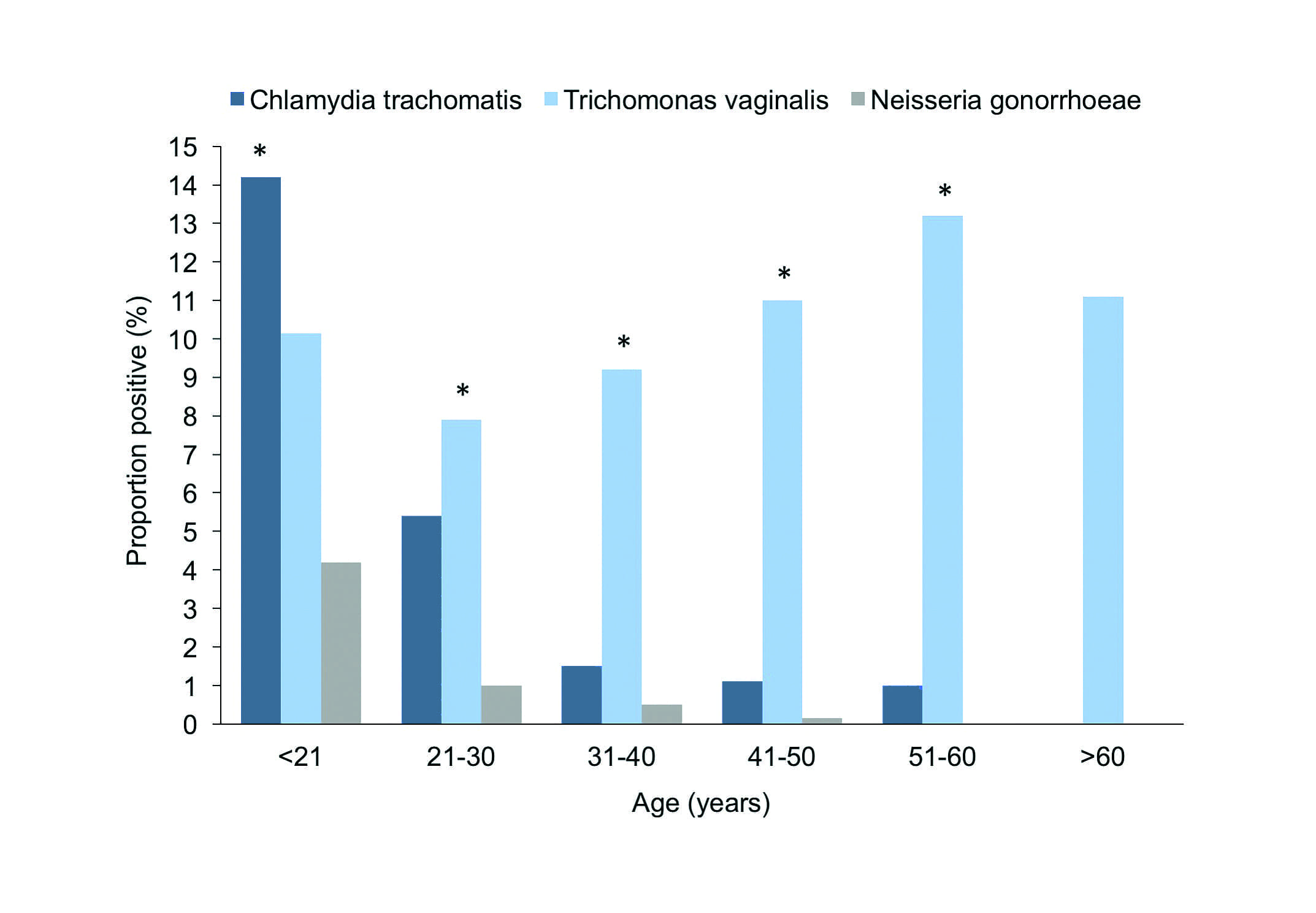
Figure 1. Prevalence of Trichomonas vaginalis, Chlamydia trachomatis, and Neisseria gonorrhoeae among 7,277 females screened using a nucleic acid amplification test, by age group. * = comparisons between T. vaginalis and C. trachomatis detection rates in which P was ?0.05. Adapted from Munson et al.3
Prevalence and Public Health Reporting
Trichomoniasis, caused by the parasite T. vaginalis, is the most prevalent nonviral STI, with an estimated 143 million new cases worldwide and 3.7 million new cases in the United States each year.1,2 While STIs are typically most prevalent among young people, the incidence of trichomoniasis appears to increase with age. In a study of 7,277 women residing in an area with a high prevalence of STIs, for example, Chlamydia trachomatis was the most prevalent STI among women aged less than 20 years, but T. vaginalis was the most prevalent STI among women aged 21 years or more, with the disparity in prevalence increasing with increasing age (Figure 1).
Aside from the general age trend, however, such estimates must be taken with a grain of salt, because the prevalence of trichomoniasis has been underestimated for several reasons. First, testing for trichomoniasis among asymptomatic patients is currently recommended only for HIV-positive women; since roughly 80% of T. vaginalis infection cases are asymptomatic, testing is frequently not undertaken and diagnoses are missed.1,4 Second, screening for trichomoniasis is performed using tests with limited sensitivity, including wet mount microscopy (sensitivity 51% to 65%), culture of vaginal specimens (75% to 96%), antigen detection (78% to 84%), and nucleic acid hybridization (roughly 60%).3–6 Finally, reporting of trichomoniasis is not mandatory in the United States; hence, even if diagnostic tests are performed and a positive diagnosis is obtained, prevalence estimates do not capture the true frequency of trichomoniasis because of underreporting.7
Thus, even though the prevalence of trichomoniasis exceeds the rate of gonorrheal and chlamydial infections combined, there is underutilization of sensitive and specific diagnostics and a lack of reporting protocols for T. vaginalis like those that already exist for Neisseria gonorrhoeae and C. trachomatis.8,9
Clinical and Public Health Implications
The absence of a reporting requirement for T. vaginalis may make sense to some clinicians who think of trichomoniasis as a ‘nuisance infection’ rather than a risk factor for serious and potentially costly negative health outcomes. In actuality, trichomoniasis represents a serious public health issue, and failure to accurately diagnose and treat trichomoniasis has serious health consequences, particularly among women.
Negative effects of T. vaginalis infection include poor pregnancy outcomes, such as low birth weight and premature delivery; a 2- to 3-fold increase in the risk of becoming HIV infected; a 2- to 3-fold increase in the risk of pelvic inflammatory disease among HIV-infected women; and persistence of high-risk human papilloma virus infection, which in turn increases the risk of cervical cancer.1,4
The public health impact of undiagnosed trichomoniasis may not be readily apparent because trichomoniasis is something of a stealth infection. Most cases are asymptomatic, and serious adverse outcomes occur primarily among pregnant women and individuals at high risk for sexually transmitted diseases. However, trichomoniasis is also highly communicable, with an estimated 14% to 60% of infected women and 60% to 100% of infected men transmitting the infection to their sexual partners.7 As a result, undiagnosed trichomoniasis can easily find its way from asymptomatic individuals to people in whom the infection may be harmful.
Fortunately, trichomoniasis is also easily treatable once diagnosed, so its spread can be reduced if effective screening protocols are in place and the reporting of positive test results becomes mandatory.
Current Testing Options
Microscopic evaluation of wet mount preparations is the most commonly employed method for diagnosing T. vaginalis infections because it is inexpensive and relatively convenient. However, wet mount methods offer low sensitivity in vaginal specimens (51% to 65%), and even lower sensitivity in semen, urethral, and urine specimens from men. Moreover, wet mount samples must be tested immediately, because they degrade by up to 20% within 10 minutes of collection.4
Culture-based testing offers better sensitivity (75% to 96%), but there are fewer options with respect to the types of samples that can be used. In women, vaginal secretions should be used, as urine samples offer less sensitivity. In men, semen samples, urethral swabs, or urine sediment are used, but it may be necessary to obtain multiple specimens from men to prepare a single culture.
Two rapid point-of-care tests that do not require the presence of viable organisms to detect T. vaginalis have received FDA clearance for the assessment of vaginal secretions. The OSOM trichomoniasis rapid test by Sekisui Diagnostics, Lexington, Mass, offers 75% to 83% sensitivity; while the Affirm VPIII microbial identification system by BD, Franklin Lakes, NJ, offers only 63% sensitivity. These tests offer a modest improvement in reliability versus wet mount tests, and are more convenient than culture tests; but optimizing both sensitivity and convenience remains a priority. The user must also be cognizant of the reference methods utilized in some of the aforementioned studies and the potential translation of performance characteristics in the face of a molecular standard.

Figure 2. The Aptima Trichomonas vaginalis assay by Hologic, Marlborough, Mass, offers 95% to 100% sensitivity and 95% to 100% specificity.
Improved Testing Options
FDA approval of the first nucleic acid amplification test for trichomoniasis 5 years ago has paved the way for more-accurate and reliable testing compared with wet mount tests, culture, or rapid point-of-care tests.10 This test, the Aptima Trichomonas vaginalis assay by Hologic, Marlborough, Mass, offers 95% to 100% sensitivity and 95% to 100% specificity (Figure 2).4,11 Automation provides control of workflow and the potential for consolidation of multiple tests (including those for chlamydia and gonorrhea) onto fewer test platforms to improve laboratory productivity and accelerate results (Figure 3).
With the Aptima test, reliable one-time and potential follow-up testing of a single specimen can be performed over an extended period of time because samples can be stored for 30 to 60 days (depending on the collection method). These advantages can help improve laboratory productivity and operational efficiencies, and allow for validation of initial findings using residual specimens rather than requiring repeat sample collection.4

Figure 3. The Aptima Trichomonas vaginalis assay is performed on the fully automated Panther testing platform by Hologic, Marlborough, Mass.
In a 2009 study, the performance of molecular diagnostic assays was compared to the performance of wet mount microscopy and culture for the detection of T. vaginalis in 296 women and 298 men who visited an STD clinic.12 When considering infected patient status—defined as a specimen yielding a positive result from wet mount, culture, or a polymerase chain reaction (PCR)-based test for T. vaginalis—PCR-based testing demonstrated increased sensitivity compared to wet mount and culture in women, and compared to culture in men.
However, when considering a molecular-resolved algorithm—defined as a specimen yielding a positive result from wet mount, culture, a PCR-based test for T. vaginalis, or the Aptima Trichomonas vaginalis assay—the Aptima test was more sensitive than the PCR-based assay in specimens derived from both women (Table 1) and men (Table 2). Possible explanations for this difference may include the inherent robustness of RNA amplification when compared to DNA amplification, multiplicity of ribosomal RNA targets per cell for the Aptima test, and inclusion of an inhibitor-removal protocol within the Aptima test.

Table 1. Performance of diagnostic tests for T. vaginalis in 296 females, based on a molecular-revised algorithm. Adapted from Nye et al.12
Based on the relative improvement in sensitivity for nucleic acid amplification tests compared with wet mount and culture testing, 2015 guidelines from the US Centers for Disease Control and Prevention (CDC) recommend that when use of nucleic acid amplification testing is not feasible in symptomatic patients, clinicians may consider adopting an algorithm wherein a wet mount test is performed first, with confirmatory nucleic acid amplification testing if the initial wet mount results are negative.4 According to the CDC guidelines, routine testing for T. vaginalis in asymptomatic pregnant women cannot be recommended based on current evidence, except for HIV-positive expectant mothers, even though pregnancy complications are a common and clinically relevant consequence of trichomoniasis.
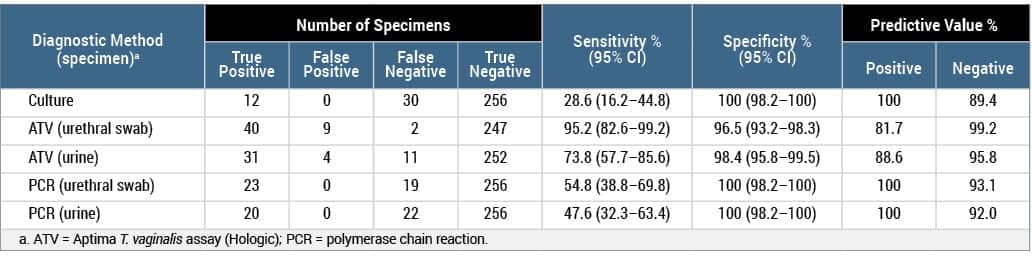
Table 2. Performance of diagnostic tests for T. vaginalis in 298 males, based on a molecular-revised algorithm. Wet mount microscopy was not evaluated because it is known to have poor sensitivity in men. Adapted from Nye et al.12
Approximately half of all HIV-infected women are coinfected with T. vaginalis, making them obvious candidates for routine testing. More accurate prevalence estimates will be necessary to identify those asymptomatic individuals for whom T. vaginalis testing would be advisable.
Cost Considerations
Ultimately, the extent to which nucleic acid amplification testing is utilized is likely to be determined in large part by cost considerations—an area that has not been extensively studied. However, a single pharmacoeconomic analysis conducted in the UK provides early clues about the cost implications of using the newer test method.13 In this analysis, use of the Aptima Trichomonas vaginalis assay for detection of T. vaginalis in 3,424 women undergoing testing for chlamydia and gonorrhea in a genitourinary clinic or primary care setting resulted in 65 additional diagnoses of trichomoniasis compared with wet mount or culture tests (97 versus 32).
The economic analysis considered two scenarios. Scenario 1 involved universal use of the same nucleic acid amplification testplatform, with the same sample, for the detection of N. gonorrhoeae, C. trachomatis, and T. vaginalis. Scenario 2 involved universal use of two different nucleic acid amplification test platforms with two separate samples—one sample to test for N. gonorrhoeae and C. trachomatis, and the other to test for T. vaginalis.
In scenario 1, the total cost of universal nucleic acid amplification testing was about £40,000 per year. The cost per positive test was £376 using the single nucleic acid amplification test platform compared to £849 for positives obtained using current microbiological testing methods (wet mount and culture). If only symptomatic women were tested, the costs per positive diagnosis were £260 and £716, respectively.
In scenario 2, the total cost of universal testing with nucleic acid amplification tests doubled to £79,700 per year. The cost per positive diagnosis was also almost doubled (data not shown). These results suggest that nucleic acid amplification testing in symptomatic patients is likely to be cost-effective, especially when the same test platform and samples collected for chlamydia and gonorrhea testing are used. More widespread deployment of this type of platform across laboratories might increase potential savings.
The pharmacoeconomic analysis found that the use of nucleic acid amplification testing among asymptomatic patients was more expensive than testing only symptomatic patients, suggesting a need to identify high-risk groups in whom routine testing in the absence of clinical indicators of infection might be cost-effective. However, limiting routine testing for STIs to individuals considered high-risk can still miss a substantial number of diagnoses. For example, risk-based testing for HIV has been shown to miss a substantial percentage of diagnoses, with the result that approximately 15% of HIV-positive individuals who are unaware of their infection transmit an estimated 40% of new HIV infections.14,15 If future research supports more widespread screening of asymptomatic patients, it is possible that additional nucleic acid amplification tests will need to be incorporated onto existing platforms in order to maximize cost-effectiveness.
To effectively utilize T. vaginalis testing, accurate prevalence estimates derived from large studies using the nucleic acid amplification platform would help to identify the high-risk populations, and would perhaps give an indication of the extent to which positive diagnoses might be obtained through more widespread or routine testing among individuals who may not be at higher risk of infection but have a substantial risk of complications if they are infected (eg, asymptomatic pregnant women). Research will also be needed to determine whether the added upfront costs of performing nucleic acid amplification tests are offset by savings from the avoidance of negative health outcomes through more reliable diagnoses. If the indication for T. vaginalis testing is found to be warranted, more widespread deployment of the nucleic acid amplification testing platform may minimize costs while maximizing diagnostic accuracy.16
Conclusion
The adoption of routine nucleic acid amplification testing and new implementation of compatible test platforms within more laboratories will result in more reliable detection of T. vaginalis infection. Prompt, reliable detection of this infection will make it possible for more patients to be treated before complications occur and help limit the spread of sexually transmitted infection.
Accurate prevalence data might help justify classification of trichomoniasis as a reportable infection, thereby informing resource allocation decisions to improve public health outcomes. Accurate prevalence estimates will also help to identify specific populations for which routine testing in asymptomatic individuals is warranted. Additional research to characterize the economic implications of widespread nucleic acid amplification testing is warranted.
Erik Munson, PhD, is affiliated with the College of Health Sciences at Marquette University. He has served as chair of American Society for Microbiology division V, and is currently an associate editor of the Journal of Clinical Microbiology. For additional information, contact CLP chief editor Steve Halasey via shalasey@medqor.
References
- Gaydos CA, Klausner JD, Pai NP, Kelly H, Coltart C, Peeling RW. Rapid and point-of-care tests for the diagnosis of Trichomonas vaginalis in women and men. Sex Transm Infect. 2017;93(S4):S31–S35; doi: 10.1136/sextrans-2016-053063.
- Stemmer SM, Mordechai E, Adelson ME, Gygax SE, Hilbert DW. Trichomonas vaginalisis most frequently detected in woman at the age of peri-/premenopause: an unusual pattern for a sexually transmitted pathogen. Am J Obstet Gynecol. 2018;218(3):328.e1–328.e13; doi: 10.1016/j.ajog.2017.12.006.
- Munson E, Kramme T, Napierala M, Munson KL, Miller C, Hryciuk JE. Female epidemiology of transcription-mediated amplification-based Trichomonas vaginalisdetection in a metropolitan setting with a high prevalence of sexually transmitted infection. J Clin Microbiol. 2012;50(12):3927–3931; doi: 10.1128/jcm.02078-12.
- Workowski KA, Bolan GA. Sexually transmitted diseases treatment guidelines, 2015. MMWR Recomm Rep. 2015;64(RR3):1–137.
- Andrea SB, Chapin KC. Comparison of Aptima Trichomonas vaginalis transcription-mediated amplification assay and BD Affirm VPIII for detection of T. vaginalis in symptomatic women: performance parameters and epidemiological implications. J Clin Microbiol. 2011;49(3):866–869; doi: 10.1128/jcm.02367-10.
- Huppert JS, Hesse E, Kim G, et al. Adolescent women can perform a point-of-care test for trichomoniasis as accurately as clinicians. Sex Trans Infect. 2010;86(7):514–519; doi: 10.1136/sti.2009.042168.
- Hoots BE, Peterman TA, Torrone EA, Weinstock H, Meites E, Bolan GA. A trich-y question: should Trichomonas vaginalis infection be reportable? Sex Transm Dis. 2013;40(2):113–116; doi: 10.1097/olq.0b013e31827c08c3.
- Hobbs MM, Seña AC. Modern diagnosis of Trichomonas vaginalis infection. Sex Transm Infect. 2013;89(6):434–438; doi: 10.1136/sextrans-2013-051057.
- National Notifiable Diseases Surveillance System (NNDSS) [online]. Atlanta: Centers for Disease Control and Prevention, 2018. Available at: wwwn.cdc.gov/nndss. Accessed October 31, 2018.
- Munson E, Miller C, Napierala M, et al. Assessment of screening practices in a subacute clinical setting following introduction of Trichomonas vaginalis nucleic acid amplification testing. WMJ. 2012;111(5):233–236.
- Aptima Trichomonas vaginalis Assay (Panther System) [instructions for use, online]. San Diego: Hologic, 2018. Available at: www.hologic.com/sites/default/files/2018-08/503684-ifu-pi_003_01.pdf. Accessed October 31, 2018.
- Nye MB, Schwebke JR, Body BA. Comparison of Aptima Trichomonas vaginalis transcription-mediated amplification to wet mount microscopy, culture, and polymerase chain reaction for diagnosis of trichomoniasis in men and women. Am J Obstet Gynecol. 2009;200(2):188.e1–188.e7; doi: 10.1016/j.ajog.2008.10.005.
- Nicholls JE, Turner KME, North P, et al. Cross-sectional study to evaluate Trichomonas vaginalis positivity in women tested for Neisseria gonorrhoeae and Chlamydia trachomatis, attending genitourinary medicine and primary care clinics in Bristol, South West England.Sex Transm Infect. 2018;94(2):93–99; doi: 10.1136/sextrans-2016-052942.
- Branson BM, Handsfield HH, Lampe MA, et al. Revised recommendations for HIV testing of adults, adolescents, and pregnant women in healthcare settings. MMWR Recomm Rep. 2006;55(RR14):1–17.
- Dailey AF, Hoots BE, Hall HI, et al. Vital signs: human immunodeficiency virus testing and diagnosis delays, United States. MMWR. 2017;66(47):1300–1306.
- Munson E. Point: new trichs for ‘old’ dogs: prospects for expansion of Trichomonas vaginalis screening. Clin Chem. 2014;60(1):151–154; doi: 10.1373/clinchem.2013.210021.




{kind=link}