
Smarter, cheaper, higher throughput—and more insights.
By Scott Powell
Throughout the past decade, demand for mid-density multiplexing technologies has increased greatly as more and more research and clinical applications have required the simultaneous testing of 5 to 50 biomarkers in a single reaction. Mid-density multiplexing applications sit between single-plex test applications, which test for 1 to 4 targets in a single reaction, and highly multiplexed test applications, which look for 50 or more targets simultaneously.
Single-plex testing is currently performed with an assortment of technologies, including real-time PCR (qPCR) molecular diagnostics and immunoassays. By contrast, highly multiplexed testing is performed with technologies such as sequencing and mass spectrometry.
There are only a handful of options for mid-density multiplexing currently available. The FilmArray System from BioFire Diagnostics, Salt Lake City; the eSensor XT-8 and ePlex systems from GenMark Diagnostics, Carlsbad, Calif; and the Verigene system from Luminex, Austin, Texas, are prominent examples. These mid-density multiplexing technologies have largely cemented this type of testing as the standard of care in countless research applications and in a wide variety of clinical applications, such as testing for bloodstream infections, gastrointestinal tract infections, and upper respiratory tract infections.
Nevertheless, penetration beyond large, well-resourced laboratories worldwide has been limited by the high instrumentation cost per test, and the limited availability of mid-density test content—a result of the complexity associated with developing such assays. To better democratize testing beyond resource-rich lab settings, laboratories are seeking solutions that will greatly reduce the costs associated with this type of testing, while streamlining mid-density multiplex test development.

Scott Powell, ChromaCode.
ChromaCode Inc, Carlsbad, Calif, is a next-generation healthcare company with a novel approach to mid-density multiplex testing, to overcome the limitations associated with current technologies in this area.
ChromaCode has developed a novel multiplexing platform called ‘high definition polymerase chain reaction’ (HDPCR) that brings together widely used, low-cost chemistries and qPCR instrumentation with proprietary data science algorithms to enable streamlined multiplex test development and very affordable test deliverables.
HDPCR seamlessly integrates with common qPCR and digital PCR (dPCR) platforms, enhancing their multiplexing levels to target 5 to 50 biomarkers without requiring any hardware changes. By leveraging the more than 80,000 qPCR and dPCR instruments already in use worldwide, ChromaCode can greatly expand access to mid-density multiplex molecular testing without burdening laboratories by adding costs for new instrumentation.
HDPCR Overview
ChromaCode’s HDPCR multiplexing technology is a novel way to expand multiplexing levels on existing qPCR and dPCR instruments without requiring modifications to the instrumentation.
Mid-density multiplexing can be achieved on a number of instruments that were previously limited to seeking 1 to 4 targets per reaction. Common examples include the Applied Biosystems 7500 Fast/Dx, and QuantStudio 5, 6, 7, and ViiA7, from Thermo Fisher Scientific, Waltham, Mass, and the LightCycler 480 II and Cobas z480 from Roche, Basel, Switzerland. Implementing the HDPCR technology requires use of the company’s proprietary HDPCR reagents and Cloud-based interpretation software, ChromaCode Cloud.
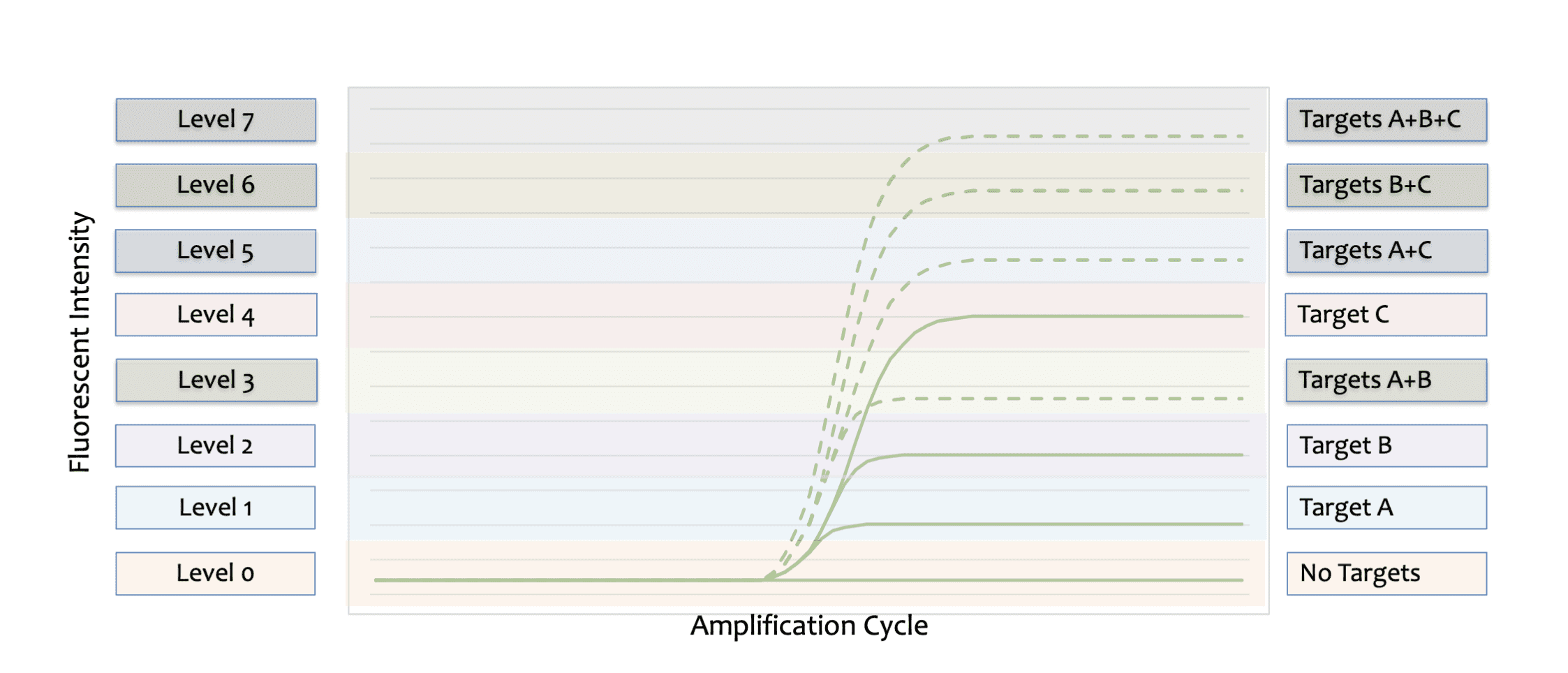
Figure 1. High definition polymerase chain reaction (HDPCR) detects multiple biomarker targets within a single color-channel by using signal intensity (brightness) to differentiate the targets. In this example, three unique targets are encoded into a single color-channel. The qPCR curves truncate into one of eight potential intensity levels, depending on what target or combination of targets is present in the sample being tested, and ranging from no targets detected (Level 0) to three targets detected (Level 7).
While multiplexing with traditional qPCR and dPCR relies on differentiation of targets by color, HDPCR encodes multiple targets into a single color channel using signal intensity to differentiate targets (Figure 1). Such differentiation is achieved, in part, by manipulation of primer and probe concentrations across targets in order to engineer predictable and reproducible curve signatures. Each HDPCR assay uses probe concentration as the limiting reagent, assigning different probe concentrations to the multiple genetic sequences being targeted within a color channel.
Since fluorescent intensity scales linearly with probe concentration within the linear dynamic range of an instrument, each target or combination of targets encoded has a distinct and predictable end-point signal intensity at reaction completion. By using signal intensity to determine which target or combination of targets is present, HDPCR effectively improves the multiplexing capability of existing qPCR and dPCR instruments instantly.
Data science plays a significant role in HDPCR technology to ensure consistent intra- and inter-instrument performance and to accelerate mid-density multiplex assay development timelines.
In order to accurately and reproducibly differentiate targets by signal intensity, HDPCR must be able to account for the noise profile unique to a given instrument—generated by thermal and optical variability—and to correct for that profile in order to ensure that accurate results are generated.
The HDPCR technology has been the subject of a series of studies that looked at the technology’s impact on reduction in coefficient of variation endpoint fluorescence, removal of crosstalk results from bleed-through between fluorescence channels, ability to detect multiple targets simultaneously across a titration series with consistent fluorescence endpoints, and sensitive copy number detection (Figure 2).1
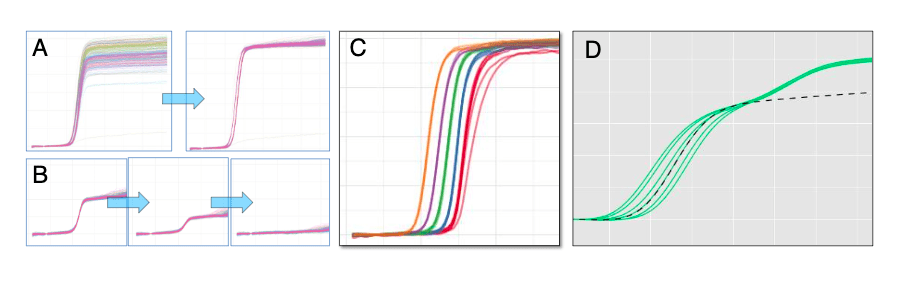
Figure 2. In the first sequence (a), a single target was tested 288 times between two operators over one week, using the high definition PCR technology by ChromaCode; after processing with the HDPCR signal processing algorithm, the coefficient of variance was 1.5%. The next sequence shows removal of FAM channel bleed-through into VIC channel (b); the raw VIC signal is shown in the first panel; the middle panel shows removal of the crosstalk signal using the instrument’s multicomponent algorithm; the last panel shows removal of the crosstalk signal using the HDPCR algorithm, illustrating a significant improvement over existing methods. The next frame (c) shows influenza A and influenza A/H3 dual-presence target titration from 10 copy input (red) to 100,000 copy input (orange). The final frame shows a dilution series for respiratory syncytial virus A (RSV A) in the presence of a very low copy number of influenza B (d); the black dotted line reflects where the fluorescence of RSV A alone would be; the green curve on top of the dotted line shows the additive signal intensity from the amplification of influenza B.
Data science is also foundational for development of the information-coding schemes needed to encode 5 to 50 target assays, across 4 to 6 color channels, on standard qPCR instruments. These schemes and the corresponding interpretive algorithms can be developed in such a way that they predict and account for common imperfections of PCR (eg, nonspecific binding, sequence drift, sequence mismatch) to ensure improved accuracy over traditional single-plex qPCR testing. This ability enables HDPCR mid-density multiplex test development to be more robust in the face of challenges that are known to plague such projects, with resulting delays in new content releases.2
Expanding Access to Test Panels
The slow development time associated with mid-density multiplex testing has limited the amount of test content available to laboratories around the world. As a result, developers have so far created mid-density multiplexing panels only for research and clinical applications judged to offer the highest volume and greatest impact. Esoteric and emerging research and clinical applications have largely been ignored. HDPCR’s data-science based approach can change this outcome by better enabling streamlined multiplexing content development, optimization, and deployment.
An example of an emerging public health challenge that has been overlooked and in need of a mid-density multiplex testing solution is tick-borne pathogens. The rapidly increasing incidence and distribution of tick-borne diseases in the United States over the past two decades has become a threat to public health (Figure 3).3
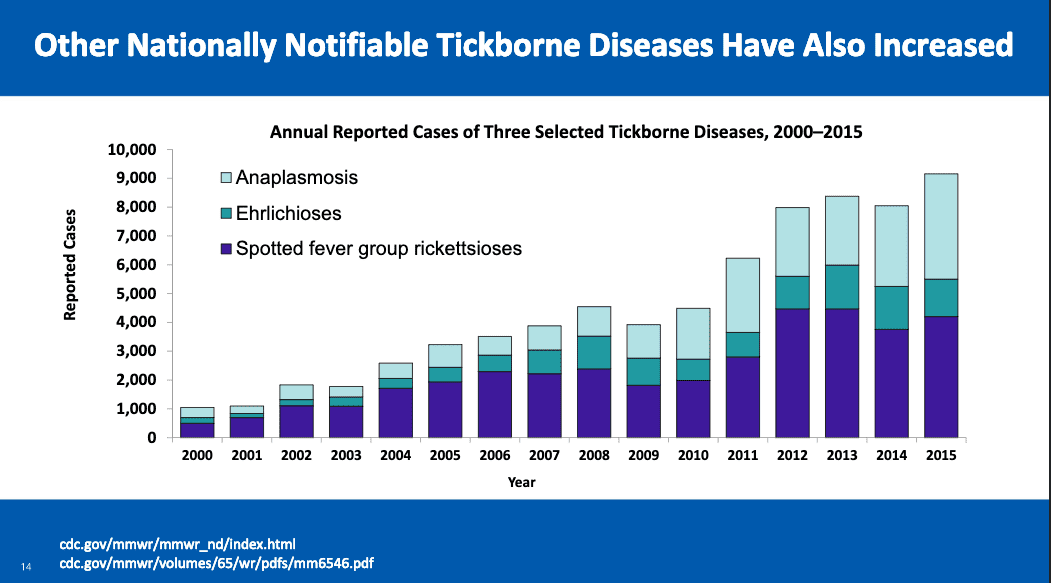
Figure 3. The incidence of tick-borne pathogens in the United States has risen dramatically over the past 25 years. According to the US Centers for Disease Control and Prevention, there have been increases of roughly 300% in the number of reported cases of Lyme disease (a), and similar increases for other nationally notifiable tick-borne diseases, including anaplasmosis, ehrlichiosis, and spotted fever group rickettsiosis (b).8
In recognition of this threat, the US Department of Health and Human Services commissioned a working group on tick-borne disease under the 21st Century Cures Act. In its initial report to Congress in late 2018, the working group noted the limitations associated with current diagnostic options—which include serologic and microscopy-based methods. The report described how such limitations can affect clinical performance and interpretation, leading to missed or incorrect diagnoses, no treatment or inappropriate treatment, increased healthcare costs, and poorer clinical outcomes. As a result, the working group recommended several initiatives for improving the ability to detect tick-borne diseases and coinfections, including:3
- Evaluate new technology or approaches for the diagnosis of Lyme disease and other tick-borne diseases.
- Fund studies and activities on tick biology and tick-borne disease ecology, including systematic tick surveillance efforts, particularly in regions beyond the Northeast and Upper Midwest.
- Fund systematic studies and activities to identify and characterize novel tick-borne disease agents in the United States.
ChromaCode launched its first multiplex HDPCR test application in December 2018: the HDCPR Tick-Borne Pathogen (TBP) panel, for research use only. The panel is a nine-target, single-well test for some of the most common tick-borne pathogens from whole blood specimens (Table 1). The test is compatible with common qPCR instrumentation and can detect tick-borne pathogens from multiple sample types, including serum and whole blood.
A recent multicenter study determined the sensitivity and specificity of HDPCR TBP to be 99.2% (94.7%–99.9%) and 99.7% (99.4%–99.9%), respectively, across 288 samples including clinical samples (n = 195) and synthetic DNA samples (n = 93).4 Of the clinical samples positive for a tick-borne pathogen, TBP achieved a sensitivity of 90.9% (10/11) for Anaplasma phagocytophilum; 100% (8/8) for Babesia microti; and 100% (1/1) for Borrelia miyamotoi.4 There were two false positive TBP results (1.0%) across the 195 clinical samples tested.4
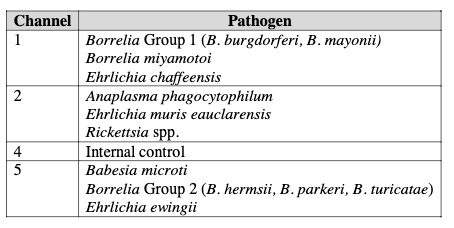
Table 1. Tick-borne pathogens detected by the HDCPR Tick-Borne Pathogen (TBP) panel from ChromaCode. The panel is a nine-target, single-well test for some of the most common tick-borne pathogens, using whole-blood specimens.
Unrivaled Quantitation, Endless Potential
Digital PCR is a very useful method for the detection and precise quantification of nucleic acid targets. Like qPCR, however, dPCR is limited in the number of targets that can be measured simultaneously in a single reaction. Despite its superior quantitative capabilities, this limitation on multiplexing has prevented dPCR from being adopted for a wider variety of clinical and research applications.
In addition to its ability to enhance the multiplexing levels of qPCR instrumentation without requiring hardware changes, ChromaCode’s HDPCR multiplexing technology is similarly able to enhance the multiplexing levels of dPCR instrumentation. By enabling highly multiplexed dPCR testing with minimal additional cost per test, ChromaCode can take advantage of the quantitative capabilities of dPCR to deliver sensitive and cost-effective testing for liquid biopsy applications targeting circulating cell-free DNA (cfDNA), including applications in noninvasive prenatal testing (NIPT) and cancer screening, diagnosis, and monitoring.
Most NIPT procedures that target cfDNA are currently performed with sequencing-based methods; but such testing has also been performed with varying degrees of success by using microarray-based or qPCR readouts. While providing the necessary performance, sequencing-based technologies are plagued by high cost, high complexity, long turnaround times, and the need for trained informatics specialists to interpret the test results. Because of these limitations, NIPT procedures have been performed mostly by large reference laboratories, and in Asia, Europe, and the United States such testing has been limited to high-risk pregnancies.5 Making such highly valuable testing available to all pregnant women globally would require a testing solution that is extremely cost-effective, high-throughput, able to generate same-day or next-day results, and capable of providing test results in a format that is easy to interpret.
In its current form, dPCR is an ideal solution for single-target testing, but it doesn’t efficiently test for the minimal 4 to 5 targets required for most NIPT applications (trisomies 13, 18, 21, and gender sexing). With the additional multiplexing provided by HDPCR methods, dPCR may quickly become a viable test methodology for cost-effective, high-throughput, and rapid turnaround time NIPT.
Like NIPT, targeting of cfDNA and circulating tumor DNA (ctDNA) for liquid biopsy cancer applications has been achieved mostly through sequencing-based methods. While the workflow and cost limitations of sequencing apply in cancer applications as in NIPT procedures, the sensitivity and comprehensiveness offered by sequencing is required for the majority of cancer testing applications.
Nevertheless, there remains ample opportunity for new testing technologies to complement sequencing tests.6 It has been shown that dPCR is capable of detecting single-nucleotide variants (SNVs), small duplications, insertions, deletions, and structural variants that cause frequently occurring breakpoints—all of which are required for oncology applications.7 Highly multiplexed dPCR testing could be a viable solution to complement sequencing-based methods as a potential front-end screening or triaging step when a discrete set of 5 to 50 biomarkers is targeted. The benefits of simplicity, improved workflow, and lower costs associated with dPCR could then expand the number of patients with access to such valuable testing.
Democratizing Mid-Density Multiplexing
Given the demonstrated value of mid-density multiplex testing, it is essential for current multiplex providers and new companies entering the field to come up with test solutions that are cost-effective and enable faster development of test content. Expansion of such testing beyond well-resourced laboratories will be limited until such barriers are overcome.
Looking toward the 2020s, the next major leap in mid-density multiplex technologies may come from companies that leverage machine learning or artificial intelligence. Using such tools to support the informatics needed to expedite assay design and optimization may lead to dramatically faster generation of content for mid-density multiplex assays.
Scott Powell is senior director for strategic marketing at ChromaCode. For further information, contact CLP chief editor Steve Halasey via [email protected].
References
- High-Definition PCR (HDPCR): Transforming Diagnostics through Data Science [white paper, online]. Carlsbad, Calif: ChromaCode, 2018. Available at: www.mlo-online.com/wp-content/uploads/2018/10/chromacode-whitepaper-rvpdemo.pdf. Accessed January 23, 2019.
- MacDonald C, Yurk D, Powell S, Rajagopal A. Comparison of Redundant Coding versus Binary Coding Scheme for Increased qPCR Multiplexing Levels and Improved Test Performance with ChromaCode’s HDPCR Platform [abstract TT069]. Poster presented at the annual meeting of the Association for Molecular Pathology, San Antonio, Texas, November 1–3, 2018. J Mol Diagn. 2018;20(6):1037; doi: 10.1016/s1525-1578(18)30401-x.
- Tick-Borne Disease Working Group: 2018 Report to Congress. Washington, DC: US Department of Health and Human Services, 2018. Available at: www.hhs.gov/sites/default/files/tbdwg-report-to-congress-2018.pdf. Accessed January 22, 2019.
- Mashock MW, Faron ML, Ledeboer NA, Buchan BW. Simultaneous Detection of Tick-Borne Pathogens Using a High-Definition Multiplexed PCR Assay [abstract ID054]. Poster presented at the annual meeting of the Association for Molecular Pathology, San Antonio, Texas, November 1–3, 2018. J Mol Diagn. 2018;20(6):951; doi: 10.1016/s1525-1578(18)30401-x.
- Kalia R, Joshi A, Dutta S, Tekchandani M, Rananaware P, Dhokar R. Noninvasive Prenatal Testing (NIPT) Market by Instruments (Ultrasound, NGS, PCR, Microarray), Consumables, Method (FCMB, cf-DNA), Application (Trisomy, Microdeletion, Genetics, Rh factor) and End-User (Hospital, Diagnostic Labs): Global Forecast to 2021. Pune, India: Markets and Markets, 2017. Available at: www.marketsandmarkets.com/market-reports/non-invasive-prenatal-testing-market-145607690.html. Accessed March 2, 2019.
- Ford A. NGS to take top spot as cancer biomarker testing broadens. CAP Today. Available at: https://captodayonline.com/ngs-take-top-spot-cancer-biomarker-testing-broadens. Accessed January 22, 2019.
- Types of Molecular Tumor Testing [online]. My Cancer Genome. Nashville: Vanderbilt-Ingram Cancer Center, 2019. Available at: www.mycancergenome.org/content/molecular-medicine/types-of-molecular-tumor-testing. Accessed January 22, 2019.
- Eisen R. Emerging Tickborne Diseases [online]. CDC Public Health Grand Rounds. Atlanta: Centers for Disease Control and Prevention, 2017. Available at: www.cdc.gov/grand-rounds/pp/2017/20170321-presentation-tickborne-diseases-h.pdf. Accessed January 22, 2019.
Featured image: Image courtesy of Adobe stock.



{kind=link}